Areefa Alladin-Karan, Susan M Samuel, Andrew W Wade, Pietro Ravani, Silviu Grisaru, Ngan N Lam, Kathryn A Bernie, Robert R Quinn
{"title":"Is Childhood IgA Nephropathy Different From Adult IgA Nephropathy? A Narrative Review.","authors":"Areefa Alladin-Karan, Susan M Samuel, Andrew W Wade, Pietro Ravani, Silviu Grisaru, Ngan N Lam, Kathryn A Bernie, Robert R Quinn","doi":"10.1177/20543581251322571","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose of the review: </strong>Immunoglobulin A (IgA) nephropathy (IgAN) is the most common primary glomerular kidney disease. Children and adults are presumed to have the same disease and are treated similarly. However, there are differences between childhood IgAN and adult IgAN that may require unique treatment considerations, even after transition to adult nephrology services. A narrative review was conducted to compare childhood and adult IgAN and to describe the distinct characteristics of childhood IgAN. Reframing childhood IgAN can inform guideline recommendations unique to childhood IgAN, the development of targeted therapies, and clinical trial design.</p><p><strong>Sources of information: </strong>Medline and Embase were searched for reports on children and adults with IgAN published between January 2013 and December 2023 (updated May 2024). The search was not restricted by age group, outcomes reported, language, or study design. Randomized controlled trials (RCTs), observational studies, review articles, and nephrology conference abstracts were included. A total of 3104 reports were retrieved. Forty-seven reports (37 primary studies and 10 reviews) were included in the review. Two RCTs and 35 observational studies included a total of 45 085 participants (9223 children and 35 862 adults).</p><p><strong>Method: </strong>Data were extracted for primary IgAN and not for IgA vasculitis-associated nephritis. Findings were described with no statistical comparisons due to variations in interventions and outcome definitions.</p><p><strong>Key findings: </strong>Gross hematuria was the obvious clinical difference between childhood IgAN and adult (60-88% vs 15-20%). Nephrotic syndrome was more common in children, approaching up to 44%, while <18% of adults had nephrotic syndrome. Children were biopsied sooner (6 vs 15 months) and had more inflammatory kidney lesions (mesangial hypercellularity: 41-82% vs 38-64%; endocapillary hypercellularity: 39-58% vs 17-34%). Chronic kidney lesions were more prevalent in adults (segmental sclerosis: 62-77% vs 8-51%; interstitial fibrosis/tubular atrophy: 34-37% vs 1-18%). The use of immunosuppressive therapy was higher in children (46-84% vs 35-56%). Children were started on immunosuppressive therapy sooner than adults. Adults were more likely to be optimized with renin-angiotensin system inhibitors (87-94% vs 49-75%). Children had better kidney function than adults at diagnosis (estimated glomerular filtration rate of 90-128 vs 50-88 ml/min/1.73 m<sup>2</sup>), and children also had better kidney survival, with kidney failure of 3.1% vs 13.4% at 5 years. Children had more risk alleles for IgAN and higher levels of mannose-binding lectin than adults.</p><p><strong>Limitations: </strong>Most studies were retrospective and observational, with limited data on children and disease mechanisms. Data were not pooled for analysis because of important differences in definitions and measurements of baseline characteristics and outcomes. Data from countries with established urine screening programs were different compared to countries without urine screening programs. Some observed differences may be due to practice variation and delayed diagnosis in adults (lead-time bias). Well-designed prospective studies and standardized measures for kidney function assessment and outcomes can reduce heterogeneity and improve results from reviews.</p><p><strong>Conclusion: </strong>Inherent differences between childhood IgAN and adult IgAN may be due to distinct disease mechanisms. Approaching childhood IgAN as a separate condition could lead to the discovery of targeted therapies and improve management during childhood and after the transition to adult care.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"12 ","pages":"20543581251322571"},"PeriodicalIF":1.5000,"publicationDate":"2025-03-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11898040/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581251322571","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose of the review: Immunoglobulin A (IgA) nephropathy (IgAN) is the most common primary glomerular kidney disease. Children and adults are presumed to have the same disease and are treated similarly. However, there are differences between childhood IgAN and adult IgAN that may require unique treatment considerations, even after transition to adult nephrology services. A narrative review was conducted to compare childhood and adult IgAN and to describe the distinct characteristics of childhood IgAN. Reframing childhood IgAN can inform guideline recommendations unique to childhood IgAN, the development of targeted therapies, and clinical trial design.
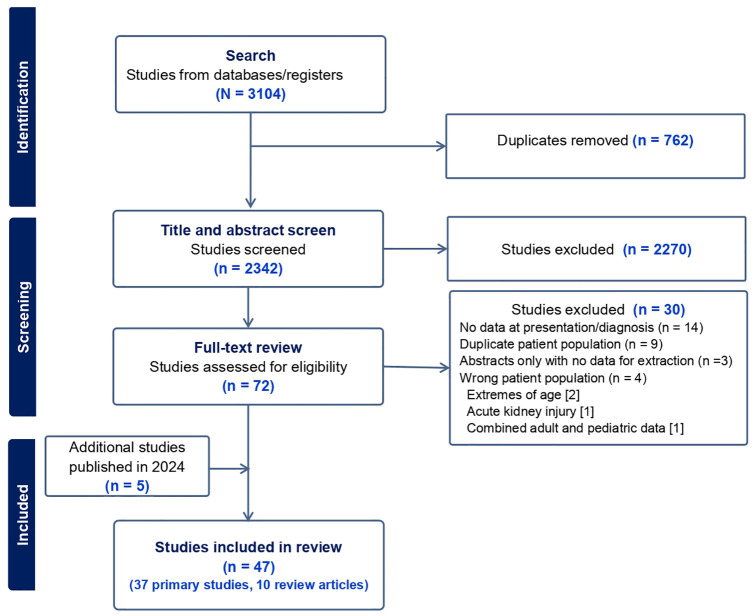
Sources of information: Medline and Embase were searched for reports on children and adults with IgAN published between January 2013 and December 2023 (updated May 2024). The search was not restricted by age group, outcomes reported, language, or study design. Randomized controlled trials (RCTs), observational studies, review articles, and nephrology conference abstracts were included. A total of 3104 reports were retrieved. Forty-seven reports (37 primary studies and 10 reviews) were included in the review. Two RCTs and 35 observational studies included a total of 45 085 participants (9223 children and 35 862 adults).
Method: Data were extracted for primary IgAN and not for IgA vasculitis-associated nephritis. Findings were described with no statistical comparisons due to variations in interventions and outcome definitions.
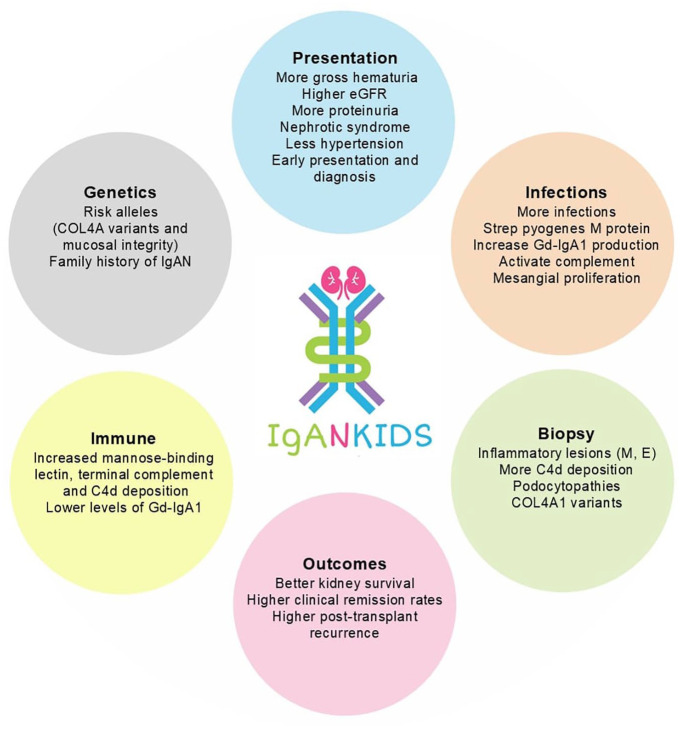
Key findings: Gross hematuria was the obvious clinical difference between childhood IgAN and adult (60-88% vs 15-20%). Nephrotic syndrome was more common in children, approaching up to 44%, while <18% of adults had nephrotic syndrome. Children were biopsied sooner (6 vs 15 months) and had more inflammatory kidney lesions (mesangial hypercellularity: 41-82% vs 38-64%; endocapillary hypercellularity: 39-58% vs 17-34%). Chronic kidney lesions were more prevalent in adults (segmental sclerosis: 62-77% vs 8-51%; interstitial fibrosis/tubular atrophy: 34-37% vs 1-18%). The use of immunosuppressive therapy was higher in children (46-84% vs 35-56%). Children were started on immunosuppressive therapy sooner than adults. Adults were more likely to be optimized with renin-angiotensin system inhibitors (87-94% vs 49-75%). Children had better kidney function than adults at diagnosis (estimated glomerular filtration rate of 90-128 vs 50-88 ml/min/1.73 m2), and children also had better kidney survival, with kidney failure of 3.1% vs 13.4% at 5 years. Children had more risk alleles for IgAN and higher levels of mannose-binding lectin than adults.
Limitations: Most studies were retrospective and observational, with limited data on children and disease mechanisms. Data were not pooled for analysis because of important differences in definitions and measurements of baseline characteristics and outcomes. Data from countries with established urine screening programs were different compared to countries without urine screening programs. Some observed differences may be due to practice variation and delayed diagnosis in adults (lead-time bias). Well-designed prospective studies and standardized measures for kidney function assessment and outcomes can reduce heterogeneity and improve results from reviews.
Conclusion: Inherent differences between childhood IgAN and adult IgAN may be due to distinct disease mechanisms. Approaching childhood IgAN as a separate condition could lead to the discovery of targeted therapies and improve management during childhood and after the transition to adult care.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


