Bunny Saberwal, Kush Patel, Ernst Klotz, Anna Herrey, Andreas Seraphim, Sebastian Vandermolen, George D Thornton, Mohammed Y Khanji, Thomas A Treibel, Francesca Pugliese
{"title":"Myocardial extracellular volume fraction by computed tomography vs. cardiovascular magnetic resonance imaging in patients with stable chest pain.","authors":"Bunny Saberwal, Kush Patel, Ernst Klotz, Anna Herrey, Andreas Seraphim, Sebastian Vandermolen, George D Thornton, Mohammed Y Khanji, Thomas A Treibel, Francesca Pugliese","doi":"10.1093/ehjimp/qyaf019","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Computed tomography (CT) is increasingly being recognized as a diagnostic modality across a range of cardiovascular conditions. Myocardial late enhancement imaging has shown value as an imaging biomarker for the identification and prognostication of disease. The objective of this study was to compare extracellular volume fraction by CT (ECVCT) against cardiovascular magnetic resonance (ECVCMR), the latter considered as reference standard for this study.</p><p><strong>Methods and results: </strong>Consecutive patients with an index history of cardiac chest pain referred for invasive angiography were prospectively recruited. In addition to late gadolinium enhancement (LGE) imaging, patients underwent 1.5 T CMR with T1-mapping [by MOdified Look-Locker Inversion (MOLLI) recovery]. Pre- and post-contrast CT was performed for whole-heart ECVCT quantification. Averaged and segmental ECVCT was compared in patients with and without LGE, as well as between mid-ventricular averaged ECVCT and ECVCMR. Bland-Altman analysis was used to determine limits of agreement and identify differences between ECVCT and ECVCMR. A total of 88 participants (74% male, mean age 59.8 ± 9.1 years) underwent ECVCT and LGE; 49 of these also underwent mid-ventricular ECVCMR. For these, the CMR and CTECV fractions were 27.6 ± 2.4 and 26.8 ± 2.2, respectively. Patients with LGE findings on CMR (<i>n</i> = 24) had a significantly higher ECVCT than those without (<i>n</i> = 64): 27.2 [25.8, 28.7] vs. 26.1 [25.0, 27.7] (<i>P</i> = 0.02). Segments with LGE demonstrated a consistently higher ECV: 30.8 [25.7, 35.9] (<i>P</i> = 0.008) (endocardial LGE) and 30.9 [27.9, 33.1] (<i>P</i> = 0.0001) (transmural LGE) vs. 26.1 [25.0, 27.4].</p><p><strong>Conclusion: </strong>ECVCT obtained from 5 min post-contrast CT protocols shows good agreement with CMR in a stable chest pain cohort. Such a protocol could be seamlessly introduced into a CT workflow for the identification of significant secondary pathologies.</p>","PeriodicalId":94317,"journal":{"name":"European heart journal. Imaging methods and practice","volume":"3 1","pages":"qyaf019"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11891481/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Imaging methods and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjimp/qyaf019","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
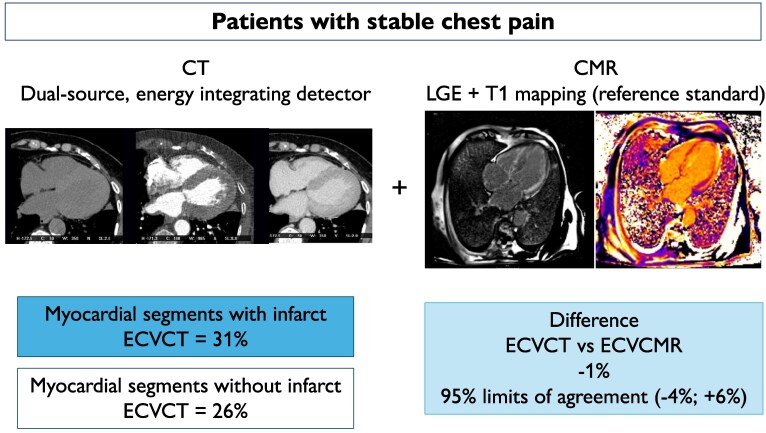
Aims: Computed tomography (CT) is increasingly being recognized as a diagnostic modality across a range of cardiovascular conditions. Myocardial late enhancement imaging has shown value as an imaging biomarker for the identification and prognostication of disease. The objective of this study was to compare extracellular volume fraction by CT (ECVCT) against cardiovascular magnetic resonance (ECVCMR), the latter considered as reference standard for this study.
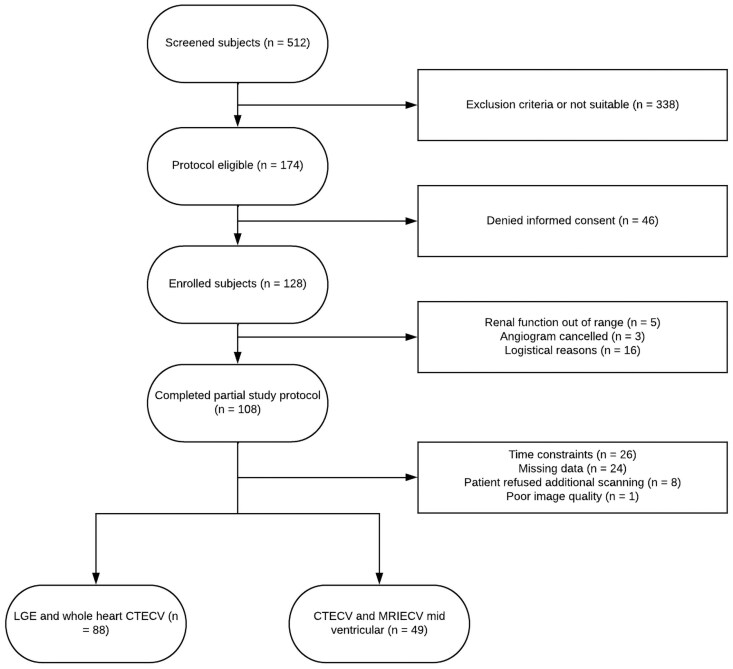
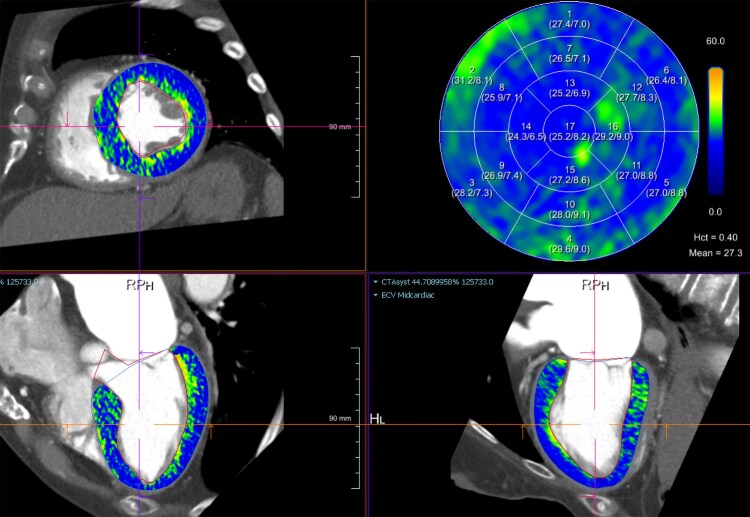
Methods and results: Consecutive patients with an index history of cardiac chest pain referred for invasive angiography were prospectively recruited. In addition to late gadolinium enhancement (LGE) imaging, patients underwent 1.5 T CMR with T1-mapping [by MOdified Look-Locker Inversion (MOLLI) recovery]. Pre- and post-contrast CT was performed for whole-heart ECVCT quantification. Averaged and segmental ECVCT was compared in patients with and without LGE, as well as between mid-ventricular averaged ECVCT and ECVCMR. Bland-Altman analysis was used to determine limits of agreement and identify differences between ECVCT and ECVCMR. A total of 88 participants (74% male, mean age 59.8 ± 9.1 years) underwent ECVCT and LGE; 49 of these also underwent mid-ventricular ECVCMR. For these, the CMR and CTECV fractions were 27.6 ± 2.4 and 26.8 ± 2.2, respectively. Patients with LGE findings on CMR (n = 24) had a significantly higher ECVCT than those without (n = 64): 27.2 [25.8, 28.7] vs. 26.1 [25.0, 27.7] (P = 0.02). Segments with LGE demonstrated a consistently higher ECV: 30.8 [25.7, 35.9] (P = 0.008) (endocardial LGE) and 30.9 [27.9, 33.1] (P = 0.0001) (transmural LGE) vs. 26.1 [25.0, 27.4].
Conclusion: ECVCT obtained from 5 min post-contrast CT protocols shows good agreement with CMR in a stable chest pain cohort. Such a protocol could be seamlessly introduced into a CT workflow for the identification of significant secondary pathologies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


