Improving pain, function and quality of life in end-stage knee osteoarthritis: a patient-preference cohort study on whole-body vibration and exercise as bridging therapies for total knee replacement.
Kendrew Yu-Hei Choi, Wai-Wang Chau, Linda Man-Kuen Li, Sammie Yuk-Lam Ng, Boie Po-Yee Lo, Michael Tim-Yun Ong, Patrick Shu-Hang Yung
{"title":"Improving pain, function and quality of life in end-stage knee osteoarthritis: a patient-preference cohort study on whole-body vibration and exercise as bridging therapies for total knee replacement.","authors":"Kendrew Yu-Hei Choi, Wai-Wang Chau, Linda Man-Kuen Li, Sammie Yuk-Lam Ng, Boie Po-Yee Lo, Michael Tim-Yun Ong, Patrick Shu-Hang Yung","doi":"10.1186/s42836-025-00301-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>End-stage knee osteoarthritis (OA) patients awaiting total knee replacement (TKR) often experience prolonged wait times and worsening symptoms. Whole-body vibration (WBV) has shown potential benefits in OA management. This study compared the efficacy of supervised exercise therapy alone and combined with WBV in reducing pain and improving function in this population.</p><p><strong>Methods: </strong>In this prospective cohort study, 555 patients with end-stage knee OA awaiting TKR were allocated to three groups: Exercise (n = 227), Exercise + WBV (n = 127), and Control (n = 201). The Exercise and Exercise + WBV groups underwent an 8-week intervention comprising strength and flexibility exercises. Primary outcomes were pain (Numeric Pain Rating Scale, NPRS) and function (Knee Injury and Osteoarthritis Outcome Score, KOOS). Outcomes were assessed at baseline and after the final treatment session. Statistical analysis included ANOVA with post-hoc Bonferroni correction for baseline comparisons and paired t-tests for longitudinal comparisons. Minimal Clinically Important Difference (MCID) and Minimal Detectable Change (MDC) were calculated to assess the clinical significance of the results.</p><p><strong>Results: </strong>Both exercise modalities significantly reduced knee pain from baseline to final session (P < 0.001). The Exercise + WBV group showed a larger reduction in NPRS score (mean ± standard deviation (SD); from 5.57 ± 1.82 to 4.65 ± 2.15) compared to the Exercise group (from 5.35 ± 2.11 to 4.88 ± 1.96), exceeding both MCID (0.94 vs. 0.45) and MDC (0.34 vs. 0.27) thresholds. The Exercise + WBV group demonstrated significant improvements in KOOS subscales (KOOS-KP: 54.31 ± 16.95 to 60.04 ± 17.13, P < 0.001; KOOS-S: 57.27 ± 19.56 to 60.50 ± 18.07, P = 0.033; KOOS-ADL: 66.99 ± 19.42 to 71.52 ± 16.32, P = 0.003), while the Exercise group did not. These improvements in KOOS subscales met or exceeded the MDC (ranging from 2.42 to 3.99) but showed variable clinical significance relative to MCID (- 0.49 to 0.04). The Exercise + WBV group also showed significant improvement in knee ROM (110.68° ± 16.52° to 115.43° ± 18.59°, P < 0.001), while the Exercise group did not.</p><p><strong>Conclusion: </strong>Both interventions effectively reduced pain and improved function in end-stage knee OA patients awaiting TKR, with the addition of WBV leading to greater improvements in several outcomes. Particularly in pain reduction, changes exceeded both MCID and MDC thresholds, suggesting WBV's potential as a clinically valuable adjunct to exercise therapy. While some improvements in functional outcomes were statistically significant and surpassed MDC values, their clinical significance varied, future research should focus on optimizing WBV protocols and investigating long-term effects to guide clinical practice in managing patients awaiting TKR.</p>","PeriodicalId":52831,"journal":{"name":"Arthroplasty","volume":"7 1","pages":"16"},"PeriodicalIF":4.3000,"publicationDate":"2025-03-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11892224/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Arthroplasty","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s42836-025-00301-6","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: End-stage knee osteoarthritis (OA) patients awaiting total knee replacement (TKR) often experience prolonged wait times and worsening symptoms. Whole-body vibration (WBV) has shown potential benefits in OA management. This study compared the efficacy of supervised exercise therapy alone and combined with WBV in reducing pain and improving function in this population.
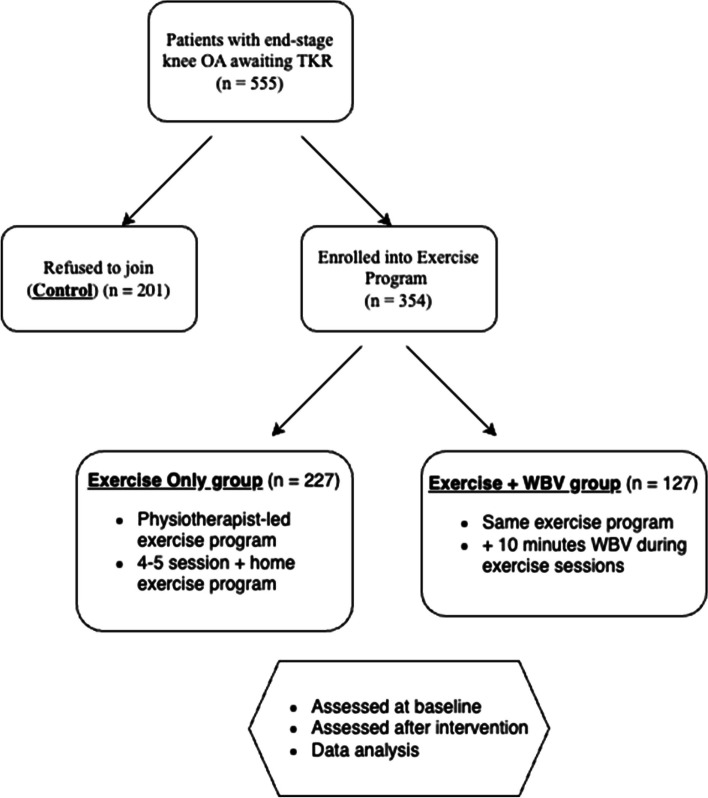
Methods: In this prospective cohort study, 555 patients with end-stage knee OA awaiting TKR were allocated to three groups: Exercise (n = 227), Exercise + WBV (n = 127), and Control (n = 201). The Exercise and Exercise + WBV groups underwent an 8-week intervention comprising strength and flexibility exercises. Primary outcomes were pain (Numeric Pain Rating Scale, NPRS) and function (Knee Injury and Osteoarthritis Outcome Score, KOOS). Outcomes were assessed at baseline and after the final treatment session. Statistical analysis included ANOVA with post-hoc Bonferroni correction for baseline comparisons and paired t-tests for longitudinal comparisons. Minimal Clinically Important Difference (MCID) and Minimal Detectable Change (MDC) were calculated to assess the clinical significance of the results.
Results: Both exercise modalities significantly reduced knee pain from baseline to final session (P < 0.001). The Exercise + WBV group showed a larger reduction in NPRS score (mean ± standard deviation (SD); from 5.57 ± 1.82 to 4.65 ± 2.15) compared to the Exercise group (from 5.35 ± 2.11 to 4.88 ± 1.96), exceeding both MCID (0.94 vs. 0.45) and MDC (0.34 vs. 0.27) thresholds. The Exercise + WBV group demonstrated significant improvements in KOOS subscales (KOOS-KP: 54.31 ± 16.95 to 60.04 ± 17.13, P < 0.001; KOOS-S: 57.27 ± 19.56 to 60.50 ± 18.07, P = 0.033; KOOS-ADL: 66.99 ± 19.42 to 71.52 ± 16.32, P = 0.003), while the Exercise group did not. These improvements in KOOS subscales met or exceeded the MDC (ranging from 2.42 to 3.99) but showed variable clinical significance relative to MCID (- 0.49 to 0.04). The Exercise + WBV group also showed significant improvement in knee ROM (110.68° ± 16.52° to 115.43° ± 18.59°, P < 0.001), while the Exercise group did not.
Conclusion: Both interventions effectively reduced pain and improved function in end-stage knee OA patients awaiting TKR, with the addition of WBV leading to greater improvements in several outcomes. Particularly in pain reduction, changes exceeded both MCID and MDC thresholds, suggesting WBV's potential as a clinically valuable adjunct to exercise therapy. While some improvements in functional outcomes were statistically significant and surpassed MDC values, their clinical significance varied, future research should focus on optimizing WBV protocols and investigating long-term effects to guide clinical practice in managing patients awaiting TKR.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


