Murong Xie, Haiyan Xu, Bin Zhang, Yunqing Ye, Zhe Li, Qingrong Liu, Zhenyan Zhao, Junxing Lyu, Yongjian Wu
{"title":"[Construction of a mixed valvular heart disease-related age-adjusted comorbidity index and its predictive value for patient prognosis].","authors":"Murong Xie, Haiyan Xu, Bin Zhang, Yunqing Ye, Zhe Li, Qingrong Liu, Zhenyan Zhao, Junxing Lyu, Yongjian Wu","doi":"10.3724/zdxbyxb-2024-0400","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To create a mixed valvular heart disease (MVHD)-related age-adjusted comorbidity index (MVACI) model for predicting mortality risk of patients with MVHD.</p><p><strong>Methods: </strong>A total of 4080 patients with moderate or severe MVHD in the China-VHD study were included. The primary endpoint was 2-year all-cause mortality. A MVACI model prediction model was constructed based on the mortality risk factors identified by univariate and multivariate Cox regression analysis. Restricted cubic splines were used to assess the relationship between MVACI scores and 2-year all-cause mortality. The optimal threshold, determined by the maximum Youden index from receiver operator characteristic (ROC) curve analysis, was used to stratify patients. Kaplan-Meier method was used to calculate 2-year all-cause mortality and compared using the Log-rank test. Univariate and multivariate Cox proportional hazards models were employed to calculate hazard ratios (HR) and 95% confidence intervals (CI), evaluating the association between MVACI scores and mortality. Paired ROC curves were used to compare the discriminative ability of MVACI scores with the European System for Cardiac Operative Risk Evaluation Ⅱ(EuroSCORE Ⅱ) or the age-adjusted Charlson comorbidity index (ACCI) in predicting 2-year clinical outcomes, while calibration curves assessed the calibration of these models. Internal validation was performed using the Bootstrap method. Subgroup analyses were conducted based on etiology, treatment strategies, and disease severity.</p><p><strong>Results: </strong>Multivariate analysis identified the following variables independently associated with 2-year all-cause mortality in patients: pulmonary hypertension, myocardiopathy, heart failure, low body weight (body mass index <18.5 kg/m<sup>2</sup>), anaemia, hypoalbuminemia, renal insufficiency, cancer, New York Heart Association (NYHA) class and age. The score was independently associated with the risk of all-cause mortality, and exhibited good discrimination (AUC=0.777, 95%<i>CI</i>: 0.755-0.799) and calibration (Brier score 0.062), with significantly better predictive performance than EuroSCORE Ⅱ or ACCI (both adjusted <i>P</i><0.01). The internal validation showed that the MVACI model's predicted probability of 2-year all-cause mortality was generally consistent with the actual probability. The AUCs for predicting all-cause mortality risk were all above 0.750, and those for predicting adverse events were all above 0.630. The prognostic value of the score remained consistent in patients regardless of their etiology, therapeutic option, and disease severity.</p><p><strong>Conclusions: </strong>The MVACI was constructed in this study based on age and comorbidities, and can be used for mortality risk prediction and risk stratification of MVHD patients. It is a simple algorithmic index and easy to use.</p>","PeriodicalId":24007,"journal":{"name":"Zhejiang da xue xue bao. Yi xue ban = Journal of Zhejiang University. Medical sciences","volume":" ","pages":"230-240"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12062937/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Zhejiang da xue xue bao. Yi xue ban = Journal of Zhejiang University. Medical sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3724/zdxbyxb-2024-0400","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To create a mixed valvular heart disease (MVHD)-related age-adjusted comorbidity index (MVACI) model for predicting mortality risk of patients with MVHD.
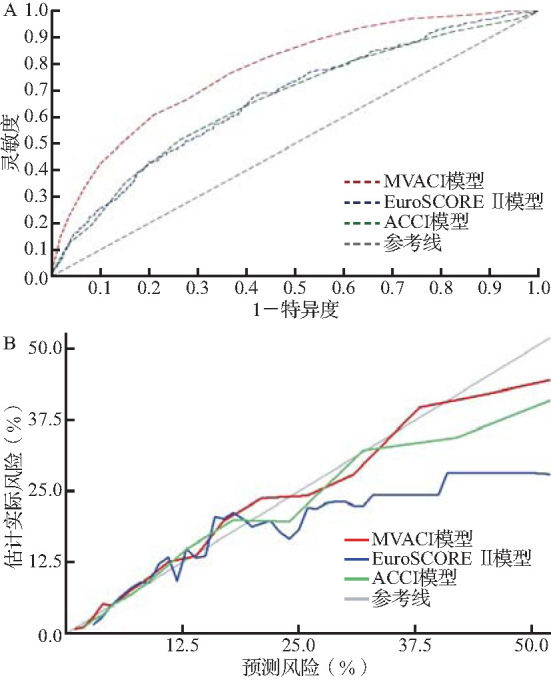
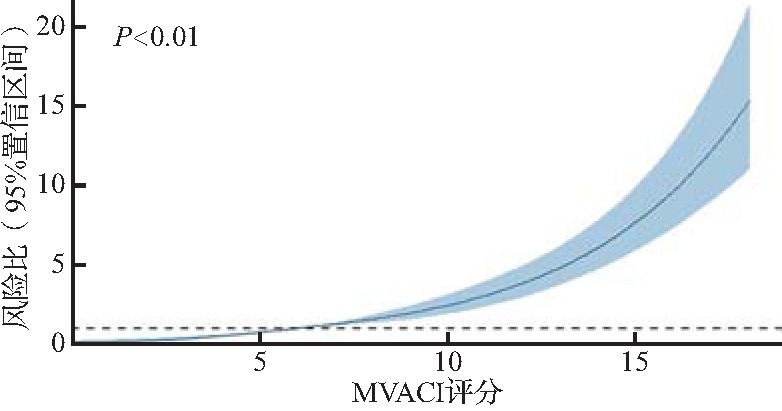
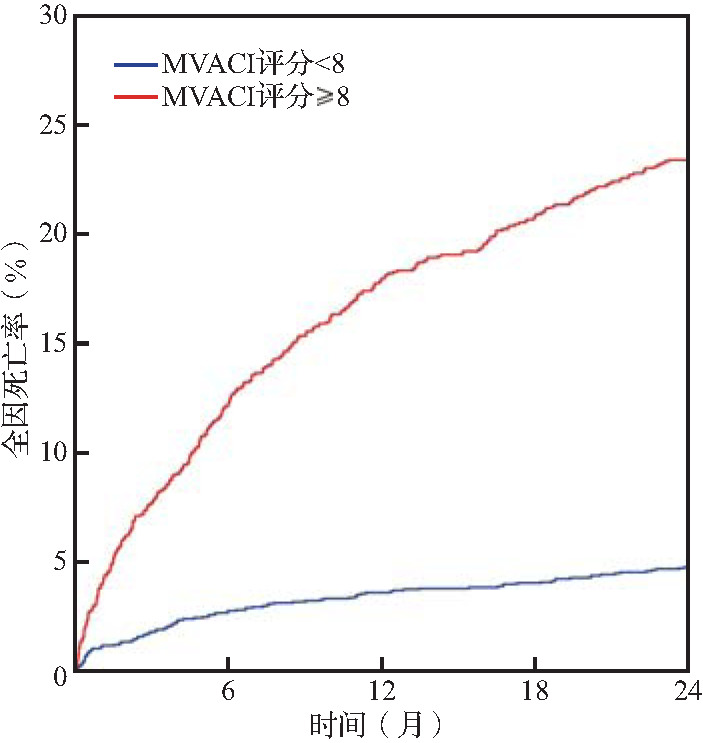
Methods: A total of 4080 patients with moderate or severe MVHD in the China-VHD study were included. The primary endpoint was 2-year all-cause mortality. A MVACI model prediction model was constructed based on the mortality risk factors identified by univariate and multivariate Cox regression analysis. Restricted cubic splines were used to assess the relationship between MVACI scores and 2-year all-cause mortality. The optimal threshold, determined by the maximum Youden index from receiver operator characteristic (ROC) curve analysis, was used to stratify patients. Kaplan-Meier method was used to calculate 2-year all-cause mortality and compared using the Log-rank test. Univariate and multivariate Cox proportional hazards models were employed to calculate hazard ratios (HR) and 95% confidence intervals (CI), evaluating the association between MVACI scores and mortality. Paired ROC curves were used to compare the discriminative ability of MVACI scores with the European System for Cardiac Operative Risk Evaluation Ⅱ(EuroSCORE Ⅱ) or the age-adjusted Charlson comorbidity index (ACCI) in predicting 2-year clinical outcomes, while calibration curves assessed the calibration of these models. Internal validation was performed using the Bootstrap method. Subgroup analyses were conducted based on etiology, treatment strategies, and disease severity.
Results: Multivariate analysis identified the following variables independently associated with 2-year all-cause mortality in patients: pulmonary hypertension, myocardiopathy, heart failure, low body weight (body mass index <18.5 kg/m2), anaemia, hypoalbuminemia, renal insufficiency, cancer, New York Heart Association (NYHA) class and age. The score was independently associated with the risk of all-cause mortality, and exhibited good discrimination (AUC=0.777, 95%CI: 0.755-0.799) and calibration (Brier score 0.062), with significantly better predictive performance than EuroSCORE Ⅱ or ACCI (both adjusted P<0.01). The internal validation showed that the MVACI model's predicted probability of 2-year all-cause mortality was generally consistent with the actual probability. The AUCs for predicting all-cause mortality risk were all above 0.750, and those for predicting adverse events were all above 0.630. The prognostic value of the score remained consistent in patients regardless of their etiology, therapeutic option, and disease severity.
Conclusions: The MVACI was constructed in this study based on age and comorbidities, and can be used for mortality risk prediction and risk stratification of MVHD patients. It is a simple algorithmic index and easy to use.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


