Lacey C Magee, Malek Bouzaher, Mihika Thapliyal, Yi-Chun Liu, Samantha Anne
{"title":"Speech Delay and Hearing Rehabilitation Disparities in Children With Hearing Loss.","authors":"Lacey C Magee, Malek Bouzaher, Mihika Thapliyal, Yi-Chun Liu, Samantha Anne","doi":"10.1002/ohn.1204","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To investigate the influence of race and insurance type on speech delay rates and hearing rehabilitation access in children with bilateral hearing loss (HL).</p><p><strong>Study design: </strong>Retrospective cross-sectional study of pediatric patients with bilateral HL who received cochlear implants (CIs) or hearing aids (HAs).</p><p><strong>Setting: </strong>This study used the national Pediatric Health Information System (PHIS) database to identify patients with HL across 52 tertiary care pediatric hospitals in the United States.</p><p><strong>Methods: </strong>Data collected included demographics, CI/HA use, speech delay/disorders, and type of insurance coverage.</p><p><strong>Results: </strong>This study identified 18,422 patients with bilateral HL (40.1% female, 66.3% white, 66.3% on public insurance), with an average age of 5.21 ± 4.37 years. Patients with private insurance were more likely to be white than non-white (48.9% vs 27.5%, P < .001), more likely to receive CI (18.0% vs 14.7%, P < .001), more likely to receive HA (21.3% vs 17.9%, P <.001), and less likely to have speech delay diagnoses (74.9% vs 81.0%, P < .001) compared to patients with public insurance. Compared to non-white patients, white patients were more likely to have CI (16.8% vs 14.7%, P < .001), more likely to have HA (20.6% vs 17.0%, P < .001), and less likely to have speech delay diagnoses (81.1% vs 77.2%, P < .001). When adjusting for other variables, these associations with insurance type and race were still observed.</p><p><strong>Conclusion: </strong>Disparities seen amongst different races and income groups can be observed at the population level and highlight an opportunity for policy interventions to secure equitable access for children with pediatric HL.</p>","PeriodicalId":19707,"journal":{"name":"Otolaryngology- Head and Neck Surgery","volume":" ","pages":"2098-2104"},"PeriodicalIF":2.5000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12120050/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Otolaryngology- Head and Neck Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/ohn.1204","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/7 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To investigate the influence of race and insurance type on speech delay rates and hearing rehabilitation access in children with bilateral hearing loss (HL).
Study design: Retrospective cross-sectional study of pediatric patients with bilateral HL who received cochlear implants (CIs) or hearing aids (HAs).
Setting: This study used the national Pediatric Health Information System (PHIS) database to identify patients with HL across 52 tertiary care pediatric hospitals in the United States.
Methods: Data collected included demographics, CI/HA use, speech delay/disorders, and type of insurance coverage.
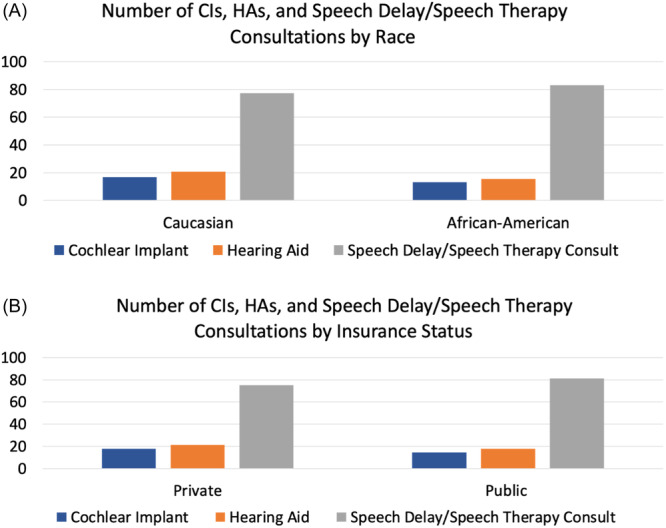
Results: This study identified 18,422 patients with bilateral HL (40.1% female, 66.3% white, 66.3% on public insurance), with an average age of 5.21 ± 4.37 years. Patients with private insurance were more likely to be white than non-white (48.9% vs 27.5%, P < .001), more likely to receive CI (18.0% vs 14.7%, P < .001), more likely to receive HA (21.3% vs 17.9%, P <.001), and less likely to have speech delay diagnoses (74.9% vs 81.0%, P < .001) compared to patients with public insurance. Compared to non-white patients, white patients were more likely to have CI (16.8% vs 14.7%, P < .001), more likely to have HA (20.6% vs 17.0%, P < .001), and less likely to have speech delay diagnoses (81.1% vs 77.2%, P < .001). When adjusting for other variables, these associations with insurance type and race were still observed.
Conclusion: Disparities seen amongst different races and income groups can be observed at the population level and highlight an opportunity for policy interventions to secure equitable access for children with pediatric HL.
目的:探讨种族和保险类型对双侧听力损失儿童言语延迟率和听力康复可及性的影响。研究设计:对接受人工耳蜗(CIs)或助听器(HAs)的双侧HL患儿进行回顾性横断面研究。背景:本研究使用国家儿童卫生信息系统(PHIS)数据库来识别美国52家三级保健儿科医院的HL患者。方法:收集的数据包括人口统计、CI/HA使用、语言延迟/障碍和保险覆盖类型。结果:本研究共发现18422例双侧HL患者(女性40.1%,白人66.3%,公保66.3%),平均年龄5.21±4.37岁。拥有私人保险的患者白人比非白人更有可能(48.9% vs 27.5%)。结论:不同种族和收入群体之间的差异可以在人口水平上观察到,并强调了政策干预的机会,以确保儿童HL患儿公平获得。
期刊介绍:
Otolaryngology–Head and Neck Surgery (OTO-HNS) is the official peer-reviewed publication of the American Academy of Otolaryngology–Head and Neck Surgery Foundation. The mission of Otolaryngology–Head and Neck Surgery is to publish contemporary, ethical, clinically relevant information in otolaryngology, head and neck surgery (ear, nose, throat, head, and neck disorders) that can be used by otolaryngologists, clinicians, scientists, and specialists to improve patient care and public health.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


