Expiratory ventilation assistance versus pressure-controlled ventilation with ambient oxygen in a hemorrhagic trauma model: a prehospital rescue option?
Tomas Karlsson, Jenny Gustavsson, Katrin Wellfelt, Mattias Günther
{"title":"Expiratory ventilation assistance versus pressure-controlled ventilation with ambient oxygen in a hemorrhagic trauma model: a prehospital rescue option?","authors":"Tomas Karlsson, Jenny Gustavsson, Katrin Wellfelt, Mattias Günther","doi":"10.1186/s40635-025-00742-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Prehospital airway management is critical for maintaining oxygenation after severe trauma hemorrhage. In cases of semi-obstructed airways, intubation with an endotracheal tube may fail, whereas a 14 French intubating catheter may provide an alternative for ventilation. Expiratory ventilation assistance (EVA) through such a catheter could serve as a prehospital rescue option, particularly when oxygen supply is limited. This study evaluates whether EVA with ambient air is sufficient to maintain oxygenation and compares its effectiveness with pressure-controlled ventilation (PCV).</p><p><strong>Methods: </strong>Twenty-three anesthetized swines (mean weight 58.3 kg, SD 4.6) were subjected to 32% blood volume hemorrhage and allocated to either EVA (n = 11) or PCV (n = 12). Historical data were used in the control group. Three phases were studied: 15 min without intervention (emulating initial prehospital care), 30 min of whole blood resuscitation, and 15 min post-resuscitation. Parameters including oxygen delivery (DO<sub>2</sub>), oxygen consumption (VO<sub>2</sub>), arterial saturation (SaO<sub>2</sub>), intratracheal pressures, and lactate levels were measured.</p><p><strong>Results: </strong>EVA and PCV demonstrated similar effectiveness in maintaining indexed DO<sub>2</sub> (p = 0.114), VO<sub>2</sub> (p = 0.325), oxygen extraction rate (p = 0.841), and SaO<sub>2</sub> (p = 0.097). Intratracheal pressures were significantly lower with EVA (p < 0.0001). EVA maintained clinically sufficient oxygenation (PaO<sub>2</sub> > 8.6 kPa) but PaCO<sub>2</sub> levels increased compared with control. Lactate levels were significantly lower in the EVA group during resuscitation (3.1 mmol/L vs. 4.8 mmol/L, p = 0.032).</p><p><strong>Conclusion: </strong>Both EVA and PCV effectively maintained oxygen delivery and sufficient oxygenation after trauma hemorrhage and whole blood resuscitation. Lower intratracheal pressures and reduced lactate accumulation with EVA suggest it may be a viable prehospital rescue method, especially in scenarios with limited oxygen supply. Further investigation is warranted to optimize its application.</p>","PeriodicalId":13750,"journal":{"name":"Intensive Care Medicine Experimental","volume":"13 1","pages":"31"},"PeriodicalIF":2.8000,"publicationDate":"2025-03-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11889277/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intensive Care Medicine Experimental","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40635-025-00742-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Prehospital airway management is critical for maintaining oxygenation after severe trauma hemorrhage. In cases of semi-obstructed airways, intubation with an endotracheal tube may fail, whereas a 14 French intubating catheter may provide an alternative for ventilation. Expiratory ventilation assistance (EVA) through such a catheter could serve as a prehospital rescue option, particularly when oxygen supply is limited. This study evaluates whether EVA with ambient air is sufficient to maintain oxygenation and compares its effectiveness with pressure-controlled ventilation (PCV).
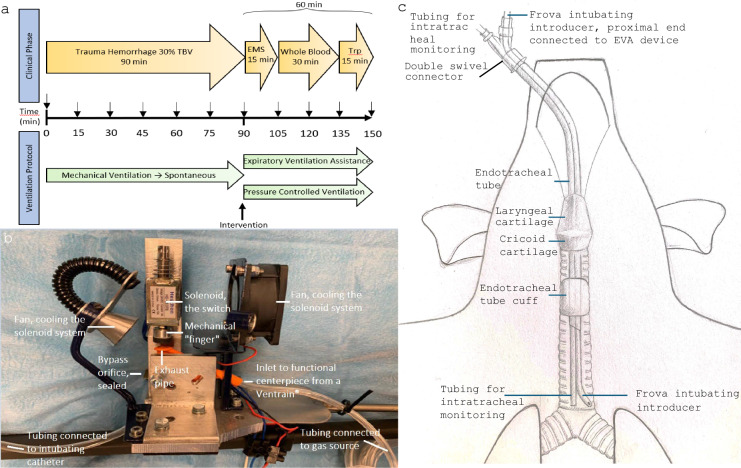
Methods: Twenty-three anesthetized swines (mean weight 58.3 kg, SD 4.6) were subjected to 32% blood volume hemorrhage and allocated to either EVA (n = 11) or PCV (n = 12). Historical data were used in the control group. Three phases were studied: 15 min without intervention (emulating initial prehospital care), 30 min of whole blood resuscitation, and 15 min post-resuscitation. Parameters including oxygen delivery (DO2), oxygen consumption (VO2), arterial saturation (SaO2), intratracheal pressures, and lactate levels were measured.
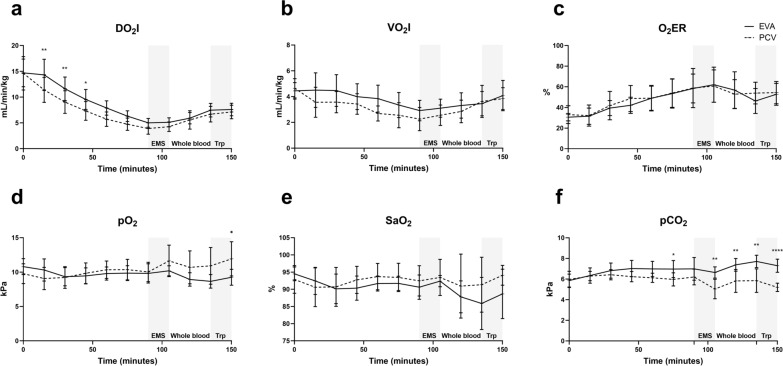
Results: EVA and PCV demonstrated similar effectiveness in maintaining indexed DO2 (p = 0.114), VO2 (p = 0.325), oxygen extraction rate (p = 0.841), and SaO2 (p = 0.097). Intratracheal pressures were significantly lower with EVA (p < 0.0001). EVA maintained clinically sufficient oxygenation (PaO2 > 8.6 kPa) but PaCO2 levels increased compared with control. Lactate levels were significantly lower in the EVA group during resuscitation (3.1 mmol/L vs. 4.8 mmol/L, p = 0.032).
Conclusion: Both EVA and PCV effectively maintained oxygen delivery and sufficient oxygenation after trauma hemorrhage and whole blood resuscitation. Lower intratracheal pressures and reduced lactate accumulation with EVA suggest it may be a viable prehospital rescue method, especially in scenarios with limited oxygen supply. Further investigation is warranted to optimize its application.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


