{"title":"Ultrasound-guided vs. Non-ultrasound-guided femoral artery puncture techniques: a comprehensive systematic review and meta-analysis.","authors":"Yi-Chen Huang, Yueh-Hsun Lu, Wei-Yi Ting","doi":"10.1186/s13089-025-00422-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To compare the effectiveness of ultrasound-guided (US) versus non-US femoral artery puncture (FAP) methods, including fluoroscopy-guided (FL) and non-guided (NG) techniques.</p><p><strong>Materials: </strong>This meta-analysis included 11 randomized controlled trials and 1 non-randomized retrospective study, comprising a total of 12 studies involving 5534 patients across diverse clinical settings. Studies varied in operator experience, institutional settings, and procedural protocols. Key outcomes assessed included complication rates, vessel access time, first-pass success rates, number of attempts, and the risk of accidental venipuncture.</p><p><strong>Results: </strong>Analysis of the heterogeneous dataset showed that guided techniques were associated with reduced complication rates compared to NG methods (pooled odds ratio (OR): 0.45, 95% Confidence Interval (CI) 0.28-0.73). US guidance was associated with decreased vessel access time (mean difference: - 16.30 s, 95% CI - 29.83 to - 2.76), higher first-pass success rates (pooled OR: 3.54, 95% CI 2.36 to 5.30), and required fewer attempts compared to non-US techniques. US guidance also showed lower risk of inadvertent venipuncture (pooled OR: 0.22, 95% CI 0.14 to 0.34).</p><p><strong>Conclusion: </strong>This meta-analysis suggests potential benefits of US femoral artery puncture techniques over non-US methods, while acknowledging significant heterogeneity across studies. The observed advantages in procedural outcomes varied across different clinical settings and operator experience levels. These findings provide setting for institutional decision-making regarding the implementation of guided puncture methods, considering factors such as operator expertise, resource availability, and specific patient populations.</p>","PeriodicalId":36911,"journal":{"name":"Ultrasound Journal","volume":"17 1","pages":"19"},"PeriodicalIF":2.9000,"publicationDate":"2025-03-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11885736/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-025-00422-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: To compare the effectiveness of ultrasound-guided (US) versus non-US femoral artery puncture (FAP) methods, including fluoroscopy-guided (FL) and non-guided (NG) techniques.
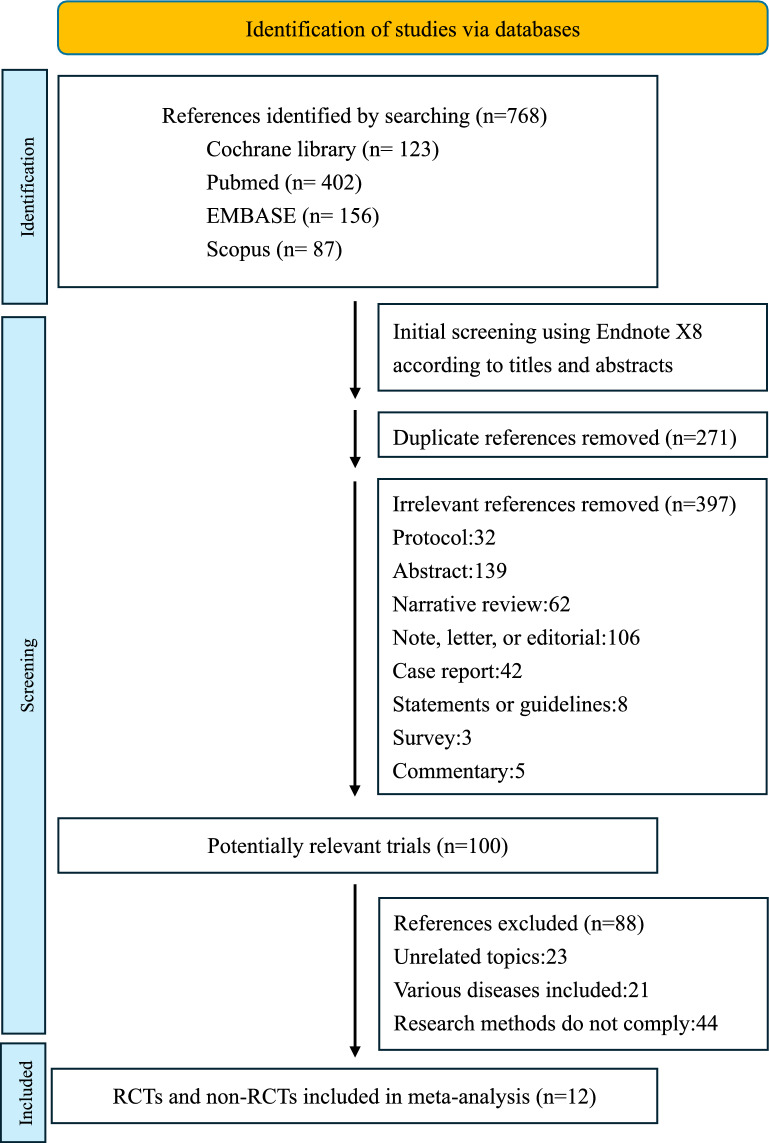
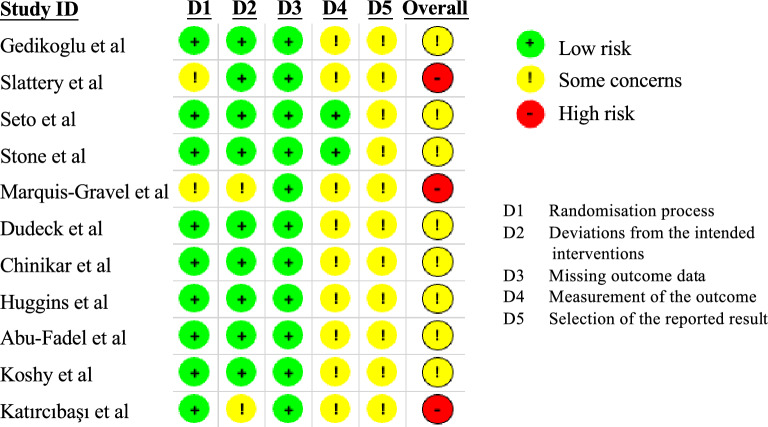
Materials: This meta-analysis included 11 randomized controlled trials and 1 non-randomized retrospective study, comprising a total of 12 studies involving 5534 patients across diverse clinical settings. Studies varied in operator experience, institutional settings, and procedural protocols. Key outcomes assessed included complication rates, vessel access time, first-pass success rates, number of attempts, and the risk of accidental venipuncture.
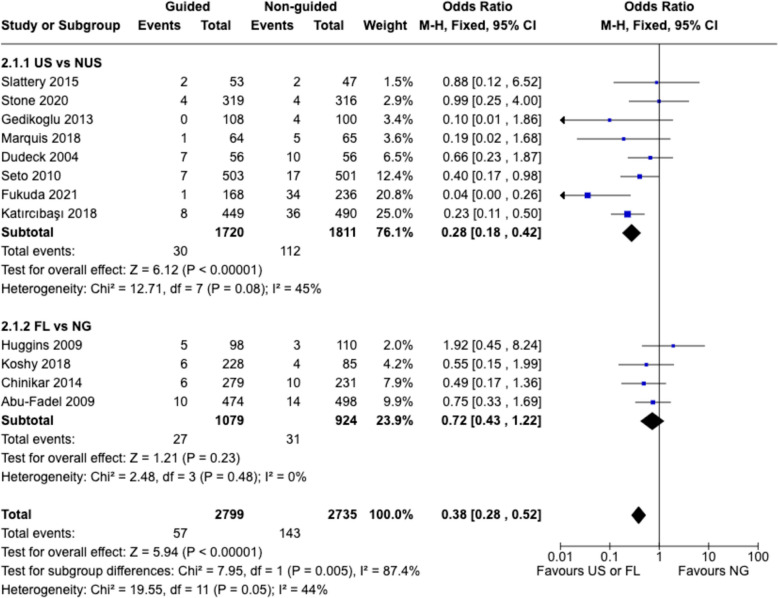
Results: Analysis of the heterogeneous dataset showed that guided techniques were associated with reduced complication rates compared to NG methods (pooled odds ratio (OR): 0.45, 95% Confidence Interval (CI) 0.28-0.73). US guidance was associated with decreased vessel access time (mean difference: - 16.30 s, 95% CI - 29.83 to - 2.76), higher first-pass success rates (pooled OR: 3.54, 95% CI 2.36 to 5.30), and required fewer attempts compared to non-US techniques. US guidance also showed lower risk of inadvertent venipuncture (pooled OR: 0.22, 95% CI 0.14 to 0.34).
Conclusion: This meta-analysis suggests potential benefits of US femoral artery puncture techniques over non-US methods, while acknowledging significant heterogeneity across studies. The observed advantages in procedural outcomes varied across different clinical settings and operator experience levels. These findings provide setting for institutional decision-making regarding the implementation of guided puncture methods, considering factors such as operator expertise, resource availability, and specific patient populations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


