Evaluation of optic nerve sheath diameter in patients undergoing robotic hysterectomy in steep Trendelenburg position compared to open abdominal hysterectomy in supine position: A randomized controlled trial.
Deepak Singla, T Mageshwaran, Yashwant S Payal, Ruma Thakuria, Kajal Shrestha
{"title":"Evaluation of optic nerve sheath diameter in patients undergoing robotic hysterectomy in steep Trendelenburg position compared to open abdominal hysterectomy in supine position: A randomized controlled trial.","authors":"Deepak Singla, T Mageshwaran, Yashwant S Payal, Ruma Thakuria, Kajal Shrestha","doi":"10.4103/joacp.joacp_348_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aims: </strong>Raised intracranial pressure (ICP) is believed to be one of the side effects of prolonged Trendelenburg position in robotic gynecologic surgeries. Optic nerve sheath diameter (ONSD) corresponds to a rise in ICP. However, the data from robotic hysterectomy surgeries is limited. So, we had planned this study with an aim to detect and compare the change in ONSD during prolonged steep Trendelenburg position in robotic hysterectomy compared to open total abdominal hysterectomy in a supine position.</p><p><strong>Material and methods: </strong>This was a prospective, observational, parallel-group, single-center study. Patients undergoing elective robotic hysterectomy and open total abdominal hysterectomy were included in this study. ONSD, end-tidal carbon dioxide (EtCO<sub>2</sub>), heart rate, and mean arterial pressure were assessed in both the groups after intubation (T0), after steep Trendelenburg position (T1), at 30 min (T2), 90 min (T3), and 180 min after docking (T4), and at the completion of surgery (de-docking) (T5). In patients undergoing open hysterectomy, the same parameters were recorded immediately after intubation (T0), at skin incision (T1), at 30 min (T2), 90 min (T3), and 180 min after skin incision (T4), and at the completion of surgery (T5).</p><p><strong>Results: </strong>Compared to the patients undergoing open hysterectomy, robotic hysterectomy patients had a significantly higher ONSD at time points T2, T3, and T4, with the maximum difference noted at the time point T4. EtCO<sub>2</sub> was higher in patients undergoing robotic hysterectomy, though the difference was significant only at time point T2. No patient in our study had any symptom or sign of raised ICP in the postoperative period.</p><p><strong>Conclusion: </strong>The steep Trendelenburg position used in robotic hysterectomy causes a significant increase in ONSD intraoperatively, and that the changes are reversible after the procedure. Further, we did not observe any complication of raised ICP postoperatively.</p>","PeriodicalId":14946,"journal":{"name":"Journal of Anaesthesiology, Clinical Pharmacology","volume":"41 1","pages":"133-139"},"PeriodicalIF":1.1000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11867365/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Anaesthesiology, Clinical Pharmacology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/joacp.joacp_348_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/23 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and aims: Raised intracranial pressure (ICP) is believed to be one of the side effects of prolonged Trendelenburg position in robotic gynecologic surgeries. Optic nerve sheath diameter (ONSD) corresponds to a rise in ICP. However, the data from robotic hysterectomy surgeries is limited. So, we had planned this study with an aim to detect and compare the change in ONSD during prolonged steep Trendelenburg position in robotic hysterectomy compared to open total abdominal hysterectomy in a supine position.
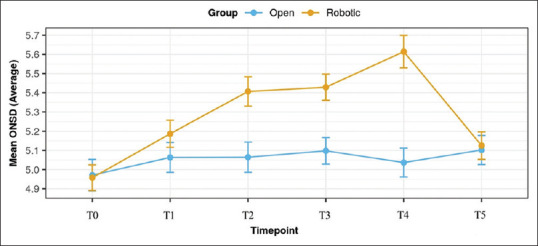
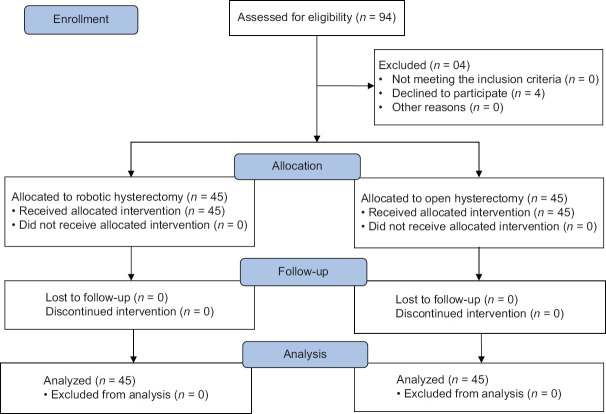
Material and methods: This was a prospective, observational, parallel-group, single-center study. Patients undergoing elective robotic hysterectomy and open total abdominal hysterectomy were included in this study. ONSD, end-tidal carbon dioxide (EtCO2), heart rate, and mean arterial pressure were assessed in both the groups after intubation (T0), after steep Trendelenburg position (T1), at 30 min (T2), 90 min (T3), and 180 min after docking (T4), and at the completion of surgery (de-docking) (T5). In patients undergoing open hysterectomy, the same parameters were recorded immediately after intubation (T0), at skin incision (T1), at 30 min (T2), 90 min (T3), and 180 min after skin incision (T4), and at the completion of surgery (T5).
Results: Compared to the patients undergoing open hysterectomy, robotic hysterectomy patients had a significantly higher ONSD at time points T2, T3, and T4, with the maximum difference noted at the time point T4. EtCO2 was higher in patients undergoing robotic hysterectomy, though the difference was significant only at time point T2. No patient in our study had any symptom or sign of raised ICP in the postoperative period.
Conclusion: The steep Trendelenburg position used in robotic hysterectomy causes a significant increase in ONSD intraoperatively, and that the changes are reversible after the procedure. Further, we did not observe any complication of raised ICP postoperatively.
期刊介绍:
The JOACP publishes original peer-reviewed research and clinical work in all branches of anaesthesiology, pain, critical care and perioperative medicine including the application to basic sciences. In addition, the journal publishes review articles, special articles, brief communications/reports, case reports, and reports of new equipment, letters to editor, book reviews and obituaries. It is international in scope and comprehensive in coverage.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


