Rima Moghnieh, Nazih Bizri, Dania Abdallah, Mohamed H Sayegh
{"title":"Antimicrobial resistance surveillance and trends in armed conflict, fragile, and non-conflict countries of the Eastern Mediterranean Region.","authors":"Rima Moghnieh, Nazih Bizri, Dania Abdallah, Mohamed H Sayegh","doi":"10.1186/s40249-025-01287-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The WHO Eastern Mediterranean Region (EMR) faces major social, economic, and demographic challenges, with nearly half of its countries affected by conflicts that severely disrupt health systems. This study compared antimicrobial resistance (AMR) rates and surveillance efforts in conflict-affected, fragile, and non-conflict countries, further subdivided by income.</p><p><strong>Methods: </strong>Data on bacteriologically confirmed bloodstream infections (BC-BSIs) from 2017 to 2021 were extracted from the WHO GLASS database. Countries were classified as conflict-affected, fragile, or non-conflict (subdivided by income) using World Bank criteria. Descriptive statistics (mean ± SD) were calculated, and group comparisons were performed using unpaired t-tests with Welch's correction. Mean differences (MD) and 95% confidence intervals (CI) were reported.</p><p><strong>Results: </strong>Conflict-affected countries reported significantly fewer surveillance sites than non-conflict countries (MD: 0.60, 95% CI: 0.361 to 0.836, P < 0.001) and fewer BC-BSIs per million population (MD: 31.00, 95% CI: 17.210 to 44.790, P < 0.001). In conflict zones, Acinetobacter spp. and S. aureus represented a higher proportion of BSIs compared to non-conflict countries (Acinetobacter spp. MD: -11.86, 95% CI: - 27.130 to 3.399, P = 0.099; S. aureus MD: - 10.68, 95% CI: - 30.030 to 8.680, P = 0.203). Carbapenem resistance in Acinetobacter spp. exceeded 65% across the groups, peaking in fragile zones (83.38%). Third-generation cephalosporin-resistant E. coli (3GCREC) prevalence ranged from 47.99% to 76.34%, peaking in conflict zones (76.34%). Carbapenem-resistant E. coli (CREC) prevalence ranged from 2.31% to 15.95%, highest in non-conflict low-middle income countries (15.95%). Third-generation cephalosporin-resistant K. pneumoniae (3GCRKP) exceeded 50% in all groups, peaking in conflict zones (80.42%). The prevalence of carbapenem-resistant K. pneumoniae (CRKP) ranged from 14.49% to 45.70%, peaking in conflict zones and non-conflict low-middle income countries (45.70%). Methicillin-resistant S. aureus (MRSA) exceeded 30%, peaking in conflict zones (70.09%).</p><p><strong>Conclusions: </strong>Conflict-affected countries have weaker AMR surveillance and lower BC-BSI detection but a higher burden of resistant pathogens, notably carbapenem-resistant Acinetobacter spp. and MRSA. Tailored strategies are essential to restore infrastructure, strengthen surveillance, and mitigate the long-term impact of AMR in these zones.</p>","PeriodicalId":48820,"journal":{"name":"Infectious Diseases of Poverty","volume":"14 1","pages":"14"},"PeriodicalIF":5.5000,"publicationDate":"2025-02-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11869426/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Diseases of Poverty","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40249-025-01287-8","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
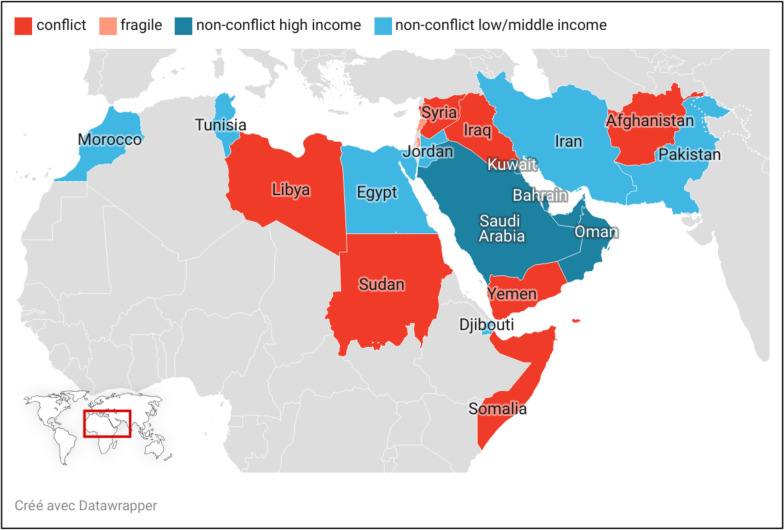
Background: The WHO Eastern Mediterranean Region (EMR) faces major social, economic, and demographic challenges, with nearly half of its countries affected by conflicts that severely disrupt health systems. This study compared antimicrobial resistance (AMR) rates and surveillance efforts in conflict-affected, fragile, and non-conflict countries, further subdivided by income.
Methods: Data on bacteriologically confirmed bloodstream infections (BC-BSIs) from 2017 to 2021 were extracted from the WHO GLASS database. Countries were classified as conflict-affected, fragile, or non-conflict (subdivided by income) using World Bank criteria. Descriptive statistics (mean ± SD) were calculated, and group comparisons were performed using unpaired t-tests with Welch's correction. Mean differences (MD) and 95% confidence intervals (CI) were reported.
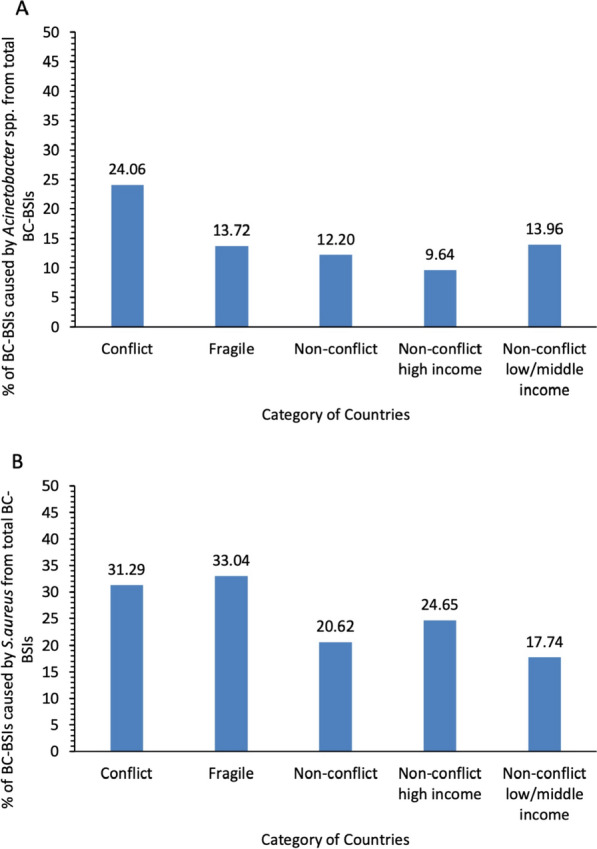
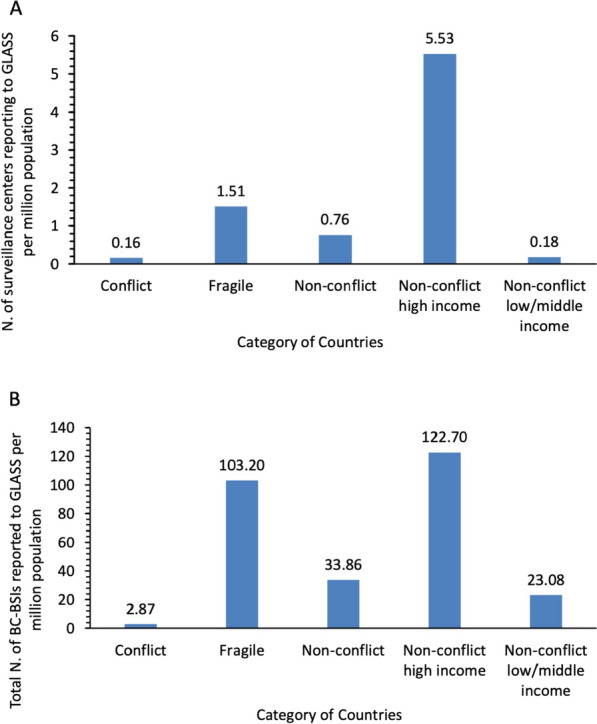
Results: Conflict-affected countries reported significantly fewer surveillance sites than non-conflict countries (MD: 0.60, 95% CI: 0.361 to 0.836, P < 0.001) and fewer BC-BSIs per million population (MD: 31.00, 95% CI: 17.210 to 44.790, P < 0.001). In conflict zones, Acinetobacter spp. and S. aureus represented a higher proportion of BSIs compared to non-conflict countries (Acinetobacter spp. MD: -11.86, 95% CI: - 27.130 to 3.399, P = 0.099; S. aureus MD: - 10.68, 95% CI: - 30.030 to 8.680, P = 0.203). Carbapenem resistance in Acinetobacter spp. exceeded 65% across the groups, peaking in fragile zones (83.38%). Third-generation cephalosporin-resistant E. coli (3GCREC) prevalence ranged from 47.99% to 76.34%, peaking in conflict zones (76.34%). Carbapenem-resistant E. coli (CREC) prevalence ranged from 2.31% to 15.95%, highest in non-conflict low-middle income countries (15.95%). Third-generation cephalosporin-resistant K. pneumoniae (3GCRKP) exceeded 50% in all groups, peaking in conflict zones (80.42%). The prevalence of carbapenem-resistant K. pneumoniae (CRKP) ranged from 14.49% to 45.70%, peaking in conflict zones and non-conflict low-middle income countries (45.70%). Methicillin-resistant S. aureus (MRSA) exceeded 30%, peaking in conflict zones (70.09%).
Conclusions: Conflict-affected countries have weaker AMR surveillance and lower BC-BSI detection but a higher burden of resistant pathogens, notably carbapenem-resistant Acinetobacter spp. and MRSA. Tailored strategies are essential to restore infrastructure, strengthen surveillance, and mitigate the long-term impact of AMR in these zones.
期刊介绍:
Infectious Diseases of Poverty is an open access, peer-reviewed journal that focuses on addressing essential public health questions related to infectious diseases of poverty. The journal covers a wide range of topics including the biology of pathogens and vectors, diagnosis and detection, treatment and case management, epidemiology and modeling, zoonotic hosts and animal reservoirs, control strategies and implementation, new technologies and application. It also considers the transdisciplinary or multisectoral effects on health systems, ecohealth, environmental management, and innovative technology. The journal aims to identify and assess research and information gaps that hinder progress towards new interventions for public health problems in the developing world. Additionally, it provides a platform for discussing these issues to advance research and evidence building for improved public health interventions in poor settings.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


