{"title":"Pembrolizumab-induced myasthenia gravis with isolated diaphragmatic involvement in a lung cancer patient: a case report.","authors":"Nefeli Mouratidou, Dimitrios Papadopoulos, Iro Vrouvaki, Vasileios Skouras, Stamatis Katsenos","doi":"10.1177/25151355251324374","DOIUrl":null,"url":null,"abstract":"<p><p>Immune-related neuromuscular disorders are rare and potentially life-threatening adverse events of immune checkpoint inhibitors (ICIs) used in the treatment of cancer. They tend to have a chronic course that usually leads to the permanent discontinuation of immunotherapy. We present a case of pembrolizumab-induced myasthenia gravis that only involved the diaphragm. The patient is a 71-year-old female with a history of stage IV lung adenocarcinoma under maintenance therapy with pemetrexed and pembrolizumab after a complete response to first-line chemo-immunotherapy. She complained of orthopnea since the previous month and was admitted due to hypoxemic respiratory failure. Radiology showed decreased lung volumes and atelectatic areas in both lower lung fields. A subsequent bronchoscopy ruled out infection and cancer recurrence. Pulmonary function tests revealed a mixed disorder with a severe reduction in maximal inspiratory pressure and a large drop in vital capacity in the supine versus the sited position. Ultrasonography of the diaphragm confirmed bilateral diaphragmatic dysfunction, and the patient was initiated on non-invasive ventilation (NIV) during sleep, which led to symptom relief. A neurological physical examination did not reveal any other muscle involvement. Laboratory tests for myasthenic syndromes showed an elevated titer of the anti-acetylcholine receptor antibody, which confirmed the diagnosis of myasthenia gravis. The patient was subsequently treated with corticosteroids, pyridostigmine, and intravenous immunoglobulin and was gradually able to wean off supplemental oxygen. On follow-up, her chest X-ray and spirometry had improved, but she continued sleeping on NIV. Pembrolizumab was stopped, and she is still free of cancer after 9 months. Clinicians treating cancer patients with immunotherapy should be aware of this rare complication and perform timely investigations in any case of orthopnea in the course of ICI therapy to offer specialized management.</p>","PeriodicalId":33285,"journal":{"name":"Therapeutic Advances in Vaccines and Immunotherapy","volume":"13 ","pages":"25151355251324374"},"PeriodicalIF":0.0000,"publicationDate":"2025-02-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11866388/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Vaccines and Immunotherapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/25151355251324374","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
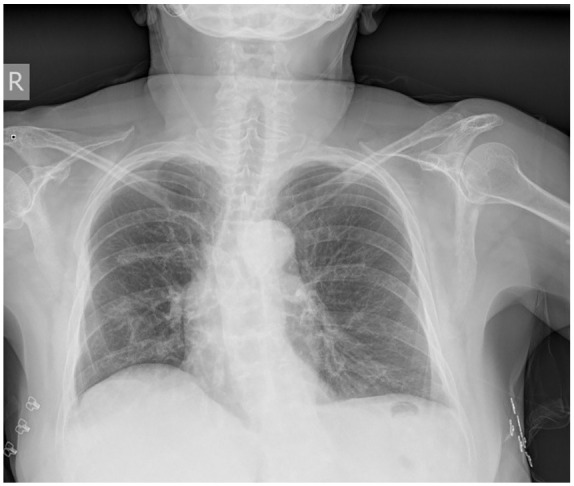
Immune-related neuromuscular disorders are rare and potentially life-threatening adverse events of immune checkpoint inhibitors (ICIs) used in the treatment of cancer. They tend to have a chronic course that usually leads to the permanent discontinuation of immunotherapy. We present a case of pembrolizumab-induced myasthenia gravis that only involved the diaphragm. The patient is a 71-year-old female with a history of stage IV lung adenocarcinoma under maintenance therapy with pemetrexed and pembrolizumab after a complete response to first-line chemo-immunotherapy. She complained of orthopnea since the previous month and was admitted due to hypoxemic respiratory failure. Radiology showed decreased lung volumes and atelectatic areas in both lower lung fields. A subsequent bronchoscopy ruled out infection and cancer recurrence. Pulmonary function tests revealed a mixed disorder with a severe reduction in maximal inspiratory pressure and a large drop in vital capacity in the supine versus the sited position. Ultrasonography of the diaphragm confirmed bilateral diaphragmatic dysfunction, and the patient was initiated on non-invasive ventilation (NIV) during sleep, which led to symptom relief. A neurological physical examination did not reveal any other muscle involvement. Laboratory tests for myasthenic syndromes showed an elevated titer of the anti-acetylcholine receptor antibody, which confirmed the diagnosis of myasthenia gravis. The patient was subsequently treated with corticosteroids, pyridostigmine, and intravenous immunoglobulin and was gradually able to wean off supplemental oxygen. On follow-up, her chest X-ray and spirometry had improved, but she continued sleeping on NIV. Pembrolizumab was stopped, and she is still free of cancer after 9 months. Clinicians treating cancer patients with immunotherapy should be aware of this rare complication and perform timely investigations in any case of orthopnea in the course of ICI therapy to offer specialized management.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


