Change in Urine Albumin-Creatinine Ratio and Occurrence of Hyperkalemia in Patients Initiating Finerenone in the USA: A Cohort Study from the FOUNTAIN Platform.
Csaba P Kovesdy, Natalie Ebert, David Vizcaya, Michael Walsh, Mikhail N Kosiborod, J Bradley Layton, Ryan Ziemiecki, Catherine B Johannes, Manel Pladevall-Vila, Patrick O Gee, Nichole Jefferson, Annie Chicoye, Maria Lopes, Bishnu Bahadur Thapa, Gary Curhan, Luis Rangel, Mudit Bhartia, Fangfang Liu, Alfredo E Farjat, Nikolaus G Oberprieler
{"title":"Change in Urine Albumin-Creatinine Ratio and Occurrence of Hyperkalemia in Patients Initiating Finerenone in the USA: A Cohort Study from the FOUNTAIN Platform.","authors":"Csaba P Kovesdy, Natalie Ebert, David Vizcaya, Michael Walsh, Mikhail N Kosiborod, J Bradley Layton, Ryan Ziemiecki, Catherine B Johannes, Manel Pladevall-Vila, Patrick O Gee, Nichole Jefferson, Annie Chicoye, Maria Lopes, Bishnu Bahadur Thapa, Gary Curhan, Luis Rangel, Mudit Bhartia, Fangfang Liu, Alfredo E Farjat, Nikolaus G Oberprieler","doi":"10.1159/000543923","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>In 2021, finerenone - a novel, selective nonsteroidal mineralocorticoid receptor antagonist - was approved in the USA to treat adults with chronic kidney disease (CKD) and type 2 diabetes (T2D). This study aimed to describe characteristics and short-term outcomes of patients prescribed finerenone since regulatory approval.</p><p><strong>Methods: </strong>This was a retrospective cohort study using claims and electronic health records data from the OM1 Real-World Data Cloud™. A total of 15,948 US adults with a previous diagnosis of CKD and T2D who initiated 10 mg or 20 mg finerenone between July 2021 and August 2023 were included. Dosing was evaluated at baseline and over up to 12-month follow-up. Change from baseline in urine albumin-to-creatinine ratio (UACR) was evaluated at 4 and 12 months (among 913 and 443 patients, respectively, with available repeat UACR values). Hyperkalemia occurrence was determined at 12 months and over total follow-up.</p><p><strong>Results: </strong>Median follow-up was 7.2 months. Mean age was 70.3 years, and 44.1% were female. At baseline (-365; 0 days), 70% had CKD stage 3; for patients with UACR measurements, 80.8% had moderate/severe albuminuria (≥30 mg/g). Median UACR was 203 mg/g. Co-medication use was ACE inhibitors/ARBs (51%), SGLT2is (38%), and GLP-1 RAs (26%). 86% of patients initiated 10 mg finerenone, and among 2,212 patients still under observation at 12 months, 70% were on 10 mg. For finerenone initiators with available UACR data, UACR was reduced by 33% at 4 months and 38% at 12 months. Hyperkalemia occurred in 1.2% of the cohort by 12 months (incidence 2.0 per 100 person-years).</p><p><strong>Conclusion: </strong>Patients who initiated finerenone had a notable reduction in median UACR at 4 months, sustained at 12 months; hyperkalemia occurrence appeared to be low. These initial findings from US clinical practice should be complemented by results from other real-world cohorts of patients started on finerenone.</p>","PeriodicalId":18998,"journal":{"name":"Nephron","volume":" ","pages":"371-383"},"PeriodicalIF":1.8000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12215156/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nephron","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000543923","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/27 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: In 2021, finerenone - a novel, selective nonsteroidal mineralocorticoid receptor antagonist - was approved in the USA to treat adults with chronic kidney disease (CKD) and type 2 diabetes (T2D). This study aimed to describe characteristics and short-term outcomes of patients prescribed finerenone since regulatory approval.
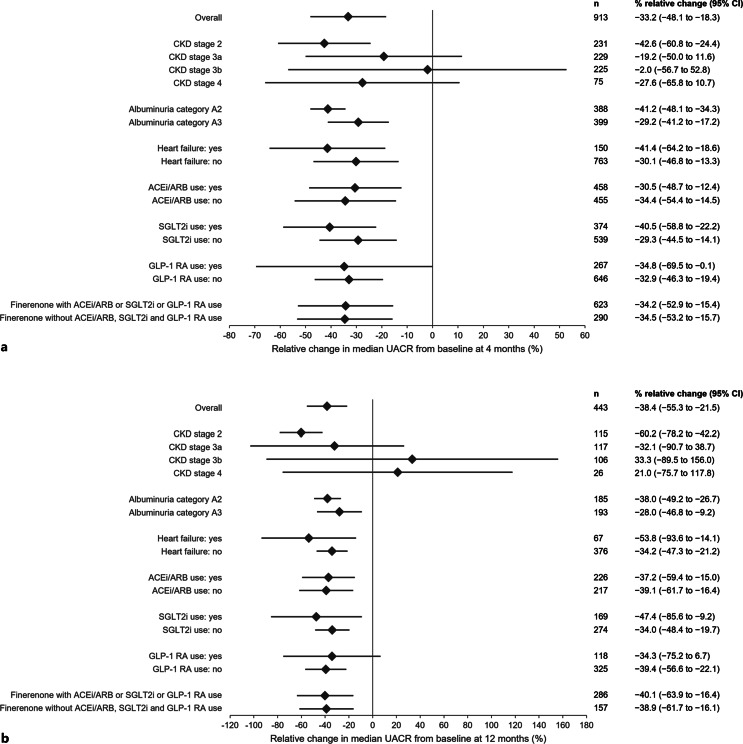
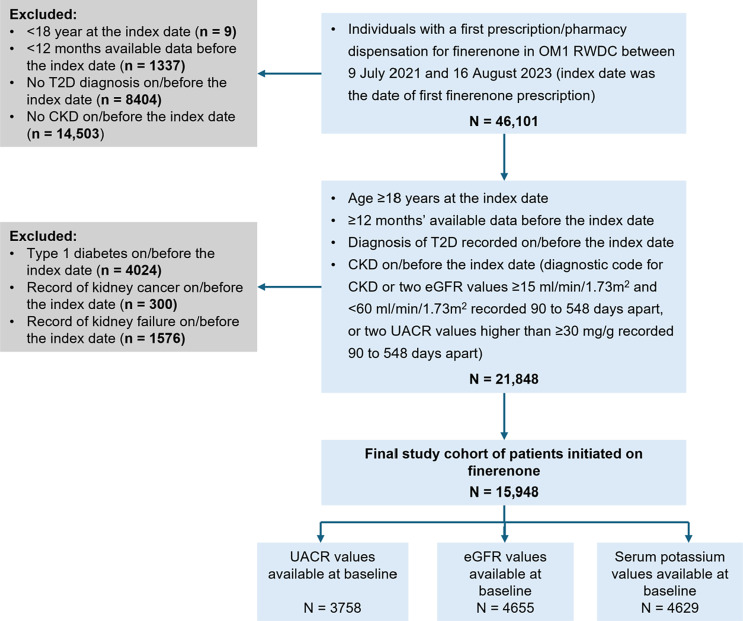
Methods: This was a retrospective cohort study using claims and electronic health records data from the OM1 Real-World Data Cloud™. A total of 15,948 US adults with a previous diagnosis of CKD and T2D who initiated 10 mg or 20 mg finerenone between July 2021 and August 2023 were included. Dosing was evaluated at baseline and over up to 12-month follow-up. Change from baseline in urine albumin-to-creatinine ratio (UACR) was evaluated at 4 and 12 months (among 913 and 443 patients, respectively, with available repeat UACR values). Hyperkalemia occurrence was determined at 12 months and over total follow-up.
Results: Median follow-up was 7.2 months. Mean age was 70.3 years, and 44.1% were female. At baseline (-365; 0 days), 70% had CKD stage 3; for patients with UACR measurements, 80.8% had moderate/severe albuminuria (≥30 mg/g). Median UACR was 203 mg/g. Co-medication use was ACE inhibitors/ARBs (51%), SGLT2is (38%), and GLP-1 RAs (26%). 86% of patients initiated 10 mg finerenone, and among 2,212 patients still under observation at 12 months, 70% were on 10 mg. For finerenone initiators with available UACR data, UACR was reduced by 33% at 4 months and 38% at 12 months. Hyperkalemia occurred in 1.2% of the cohort by 12 months (incidence 2.0 per 100 person-years).
Conclusion: Patients who initiated finerenone had a notable reduction in median UACR at 4 months, sustained at 12 months; hyperkalemia occurrence appeared to be low. These initial findings from US clinical practice should be complemented by results from other real-world cohorts of patients started on finerenone.
期刊介绍:
''Nephron'' comprises three sections, which are each under the editorship of internationally recognized leaders and served by specialized Associate Editors. Apart from high-quality original research, ''Nephron'' publishes invited reviews/minireviews on up-to-date topics. Papers undergo an innovative and transparent peer review process encompassing a Presentation Report which assesses and summarizes the presentation of the paper in an unbiased and standardized way.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


