{"title":"Is carvedilol superior to propranolol in patients with cirrhosis with portal hypertension: a systematic and meta-analysis.","authors":"Siddheesh Rajpurohit, Balaji Musunuri, Pooja Basthi Mohan, Ganesh Bhat, Shiran Shetty","doi":"10.7573/dic.2024-11-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Carvedilol has shown greater potency than propranolol as a β-blocker in managing cardiac conditions. However, its efficacy in reducing portal hypertension (PHTN) in patients with cirrhosis remains unclear. This study evaluates the efficacy and safety of carvedilol compared with propranolol in managing PHTN.</p><p><strong>Methods: </strong>A systematic review and meta-analysis were conducted using PubMed, Scopus and Embase databases. Randomized controlled trials comparing carvedilol and propranolol were included. Primary outcomes were changes in hepatic venous pressure gradient, wedge hepatic venous pressure and free hepatic venous pressure. Secondary outcomes included heart rate, cardiac output and mean arterial pressure. Tertiary outcomes assessed adverse event incidences.</p><p><strong>Results: </strong>Six randomized controlled trials involving 336 patients (171 carvedilol, 165 propranolol) were analysed. Carvedilol significantly reduced hepatic venous pressure gradient (mean difference (MD): 2.22 (95% CI 1.82-2.62); <i>p</i><0.00001) and wedge hepatic venous pressure (MD: 2.38 (95% CI 1.92-2.84); <i>p</i><0.00001). Propranolol significantly reduced cardiac output (MD: -0.60 (95% CI -0.74 to -0.45); <i>p</i><0.00001). Mean arterial pressure was significantly lower in the carvedilol group (MD: 1.79 (95% CI 0.38-3.20); <i>p</i>=0.01). Adverse events, such as orthostatic hypotension and increased diuretic use, were more frequent in the carvedilol group but were manageable.</p><p><strong>Conclusion: </strong>Carvedilol demonstrates superior efficacy in reducing PHTN compared with propranolol, with a slightly higher but tolerable adverse event profile. It may be considered the first-line treatment for PHTN. Further research is needed to validate long-term benefits and safety.</p>","PeriodicalId":11362,"journal":{"name":"Drugs in Context","volume":"14 ","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2025-02-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11867166/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drugs in Context","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7573/dic.2024-11-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Pharmacology, Toxicology and Pharmaceutics","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Carvedilol has shown greater potency than propranolol as a β-blocker in managing cardiac conditions. However, its efficacy in reducing portal hypertension (PHTN) in patients with cirrhosis remains unclear. This study evaluates the efficacy and safety of carvedilol compared with propranolol in managing PHTN.
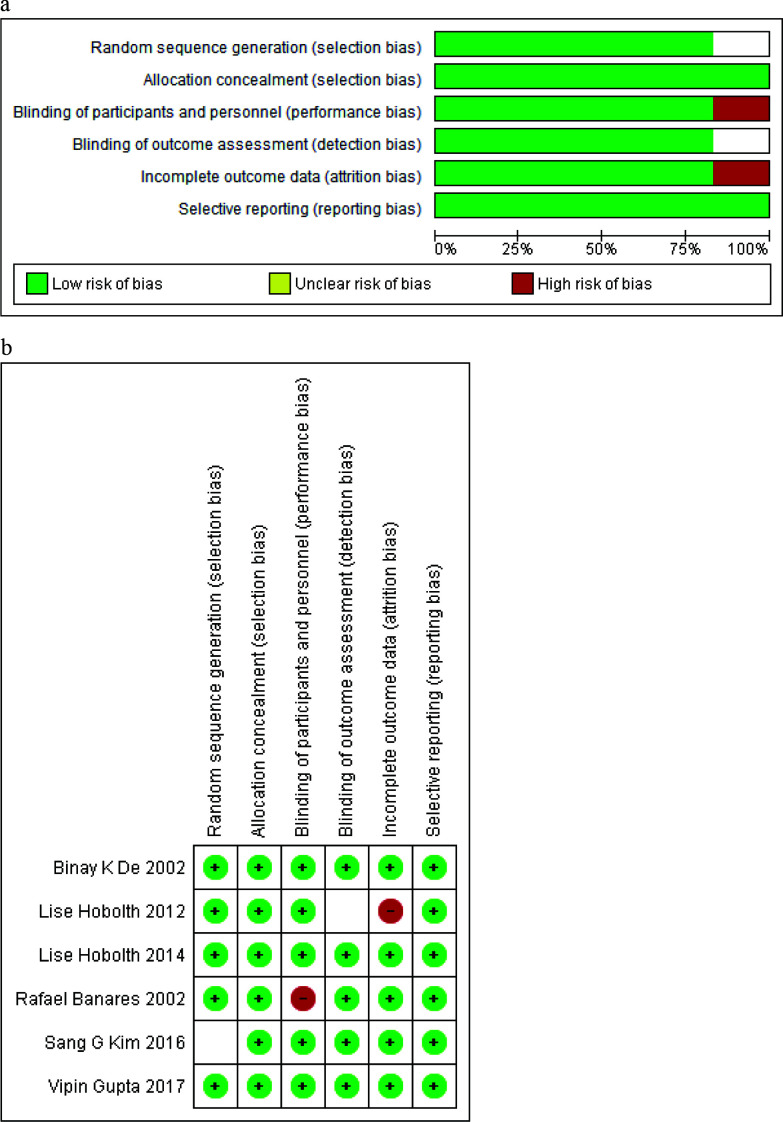
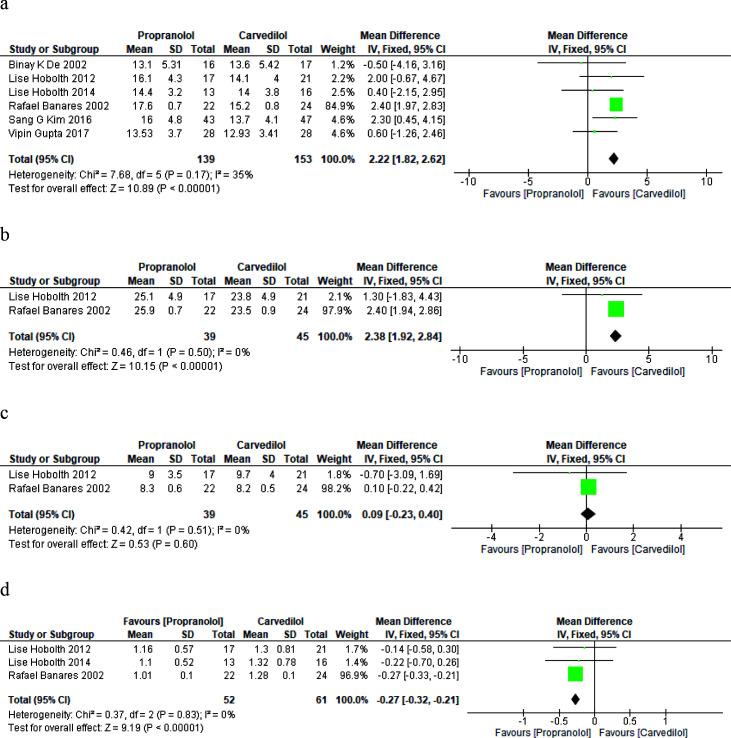
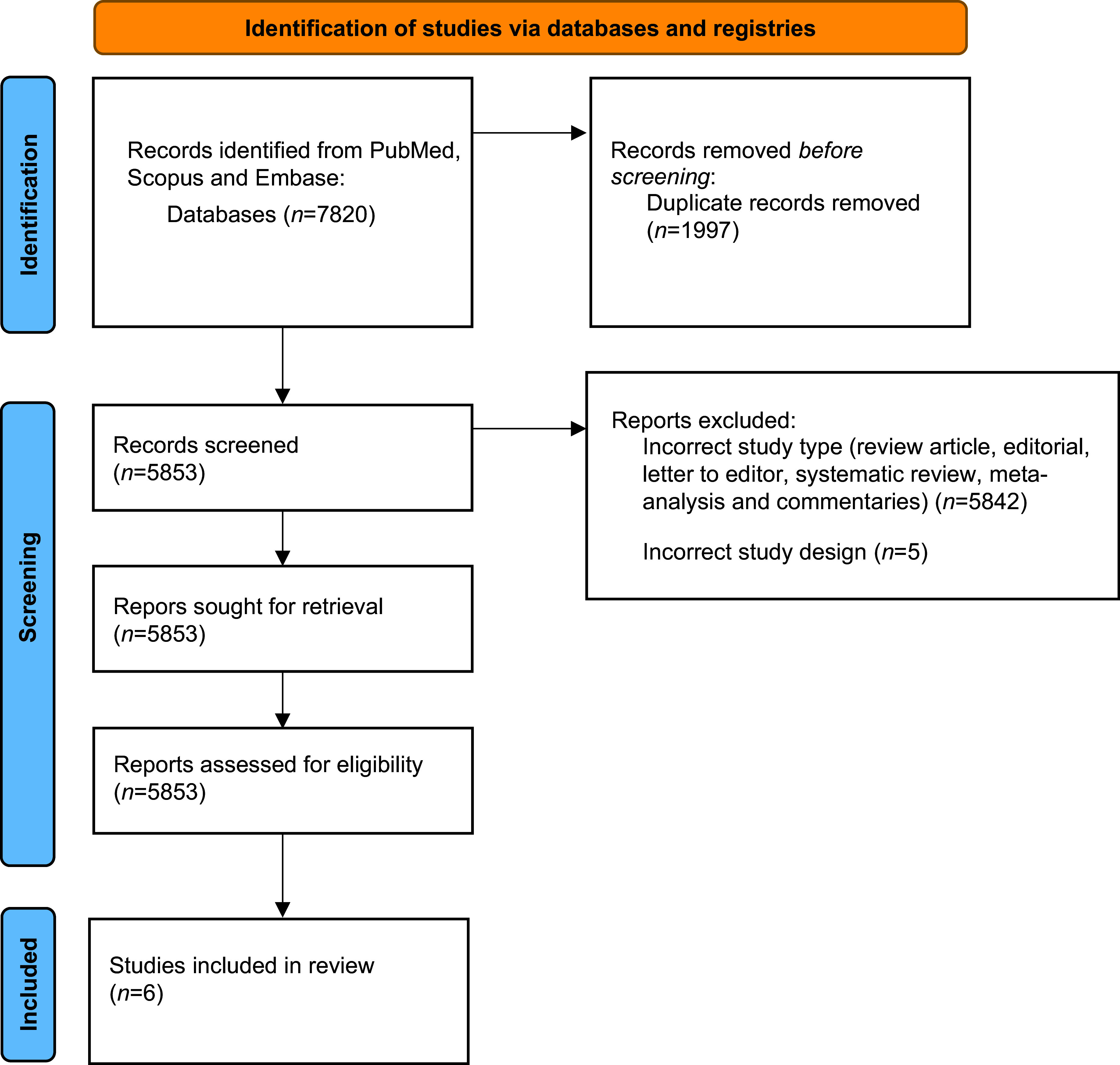
Methods: A systematic review and meta-analysis were conducted using PubMed, Scopus and Embase databases. Randomized controlled trials comparing carvedilol and propranolol were included. Primary outcomes were changes in hepatic venous pressure gradient, wedge hepatic venous pressure and free hepatic venous pressure. Secondary outcomes included heart rate, cardiac output and mean arterial pressure. Tertiary outcomes assessed adverse event incidences.
Results: Six randomized controlled trials involving 336 patients (171 carvedilol, 165 propranolol) were analysed. Carvedilol significantly reduced hepatic venous pressure gradient (mean difference (MD): 2.22 (95% CI 1.82-2.62); p<0.00001) and wedge hepatic venous pressure (MD: 2.38 (95% CI 1.92-2.84); p<0.00001). Propranolol significantly reduced cardiac output (MD: -0.60 (95% CI -0.74 to -0.45); p<0.00001). Mean arterial pressure was significantly lower in the carvedilol group (MD: 1.79 (95% CI 0.38-3.20); p=0.01). Adverse events, such as orthostatic hypotension and increased diuretic use, were more frequent in the carvedilol group but were manageable.
Conclusion: Carvedilol demonstrates superior efficacy in reducing PHTN compared with propranolol, with a slightly higher but tolerable adverse event profile. It may be considered the first-line treatment for PHTN. Further research is needed to validate long-term benefits and safety.
期刊介绍:
Covers all phases of original research: laboratory, animal and human/clinical studies, health economics and outcomes research, and postmarketing studies. Original research that shows positive or negative results are welcomed. Invited review articles may cover single-drug reviews, drug class reviews, latest advances in drug therapy, therapeutic-area reviews, place-in-therapy reviews, new pathways and classes of drugs. In addition, systematic reviews and meta-analyses are welcomed and may be published as original research if performed per accepted guidelines. Editorials of key topics and issues in drugs and therapeutics are welcomed. The Editor-in-Chief will also consider manuscripts of interest in areas such as technologies that support diagnosis, assessment and treatment. EQUATOR Network reporting guidelines should be followed for each article type. GPP3 Guidelines should be followed for any industry-sponsored manuscripts. Other Editorial sections may include Editorial, Case Report, Conference Report, Letter-to-the-Editor, Educational Section.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


