Santino R Rellum, Sijm H Noteboom, Björn J P van der Ster, Jaap Schuurmans, Eline Kho, Alexander P J Vlaar, Jimmy Schenk, Denise P Veelo
{"title":"The hypotension prediction index versus mean arterial pressure in predicting intraoperative hypotension: A clinical perspective.","authors":"Santino R Rellum, Sijm H Noteboom, Björn J P van der Ster, Jaap Schuurmans, Eline Kho, Alexander P J Vlaar, Jimmy Schenk, Denise P Veelo","doi":"10.1097/EJA.0000000000002150","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The hypotension prediction index (HPI) predicts hypotension, with randomised trials showing a significant reduction in hypotension-related metrics. However, the reliability of previous validation studies is debated, and it's unclear if mean arterial pressure (MAP) can be used interchangeably with HPI.</p><p><strong>Objectives: </strong>This study compared the effectiveness of HPI versus MAP thresholds in predicting intraoperative hypotension, focusing on three clinically relevant metrics: time from alert to event, positive predictive value (PPV), and proportion of missed hypotensive events.</p><p><strong>Design: </strong>Prospective observational study conducted between 2018 and 2020.</p><p><strong>Setting: </strong>Single-centre, academic hospital in the Netherlands.</p><p><strong>Participants: </strong>Adults scheduled for elective non-cardiac surgery lasting over two hours. Of the 105 eligible patients, 91 had sufficient data for analysis.</p><p><strong>Main outcome measures: </strong>The primary outcome was the time-to-hypotensive event intervals predicted by HPI popup alerts (≥85 for ≥40 s) and MAP-alerts (70-75 mmHg). Secondary analyses examined differences between these predictors regarding the PPV and missed event rates, as well as the difference in these metrics between instant HPI-85 alerts and the six MAP-alerts.</p><p><strong>Results: </strong>The largest time-to-event difference was seen between HPI-85 popup and MAP-70 alerts, with a gain of 0.58 (95% confidence interval (CI), 0.57 to 0.58) min, favouring HPI. Higher MAP thresholds reduced this time difference, but worsened PPV values, with 20.5 (95% CI, 20.3 to 20.6)% at MAP-75 compared to 55.6 (95% CI, 55.4 to 55.8)% for HPI-85 popups. Missed event proportions were similar: between one to three percent. Instant HPI-85 and MAP-72 alerts showed comparable performance, but both had suboptimal PPV values around 30%. However, adding a 40-s time-dependence to MAP's alert definition levelled the differences across the three evaluated metrics, aligning more closely with HPI-85 popup alerts.</p><p><strong>Conclusions: </strong>Using HPI-85 popup alerts does not provide additional prediction time over MAP-alerts in the 70 to 75 mmHg range, but they may be preferred due to higher PPV values. Instant HPI-85 and MAP-alerts perform similarly, with MAP-72 being closest, though these alerts more frequently occur regardless of subsequent hypotension with the potential to introduce unnecessary treatment. Adding a 40-s time-dependence to MAP-alerts to match the HPI popup characteristic eliminates distinctions between prediction time and missed events, while maintaining the higher PPV. However, whether 40sec-MAP-alerts are clinically equivalent remains to be determined in prospective clinical trials.</p><p><strong>Trial registration: </strong>Clinicaltrials.gov NCT03795831 on 10 January 2019.</p>","PeriodicalId":11920,"journal":{"name":"European Journal of Anaesthesiology","volume":" ","pages":"527-535"},"PeriodicalIF":6.8000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12052080/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Anaesthesiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/EJA.0000000000002150","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/27 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The hypotension prediction index (HPI) predicts hypotension, with randomised trials showing a significant reduction in hypotension-related metrics. However, the reliability of previous validation studies is debated, and it's unclear if mean arterial pressure (MAP) can be used interchangeably with HPI.
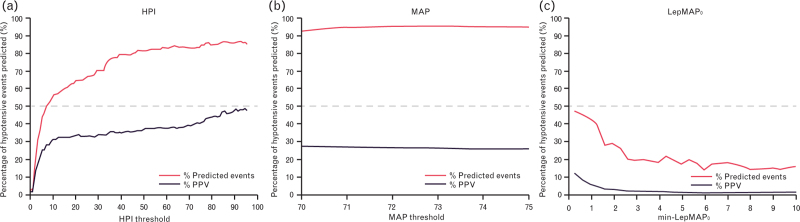
Objectives: This study compared the effectiveness of HPI versus MAP thresholds in predicting intraoperative hypotension, focusing on three clinically relevant metrics: time from alert to event, positive predictive value (PPV), and proportion of missed hypotensive events.
Design: Prospective observational study conducted between 2018 and 2020.
Setting: Single-centre, academic hospital in the Netherlands.
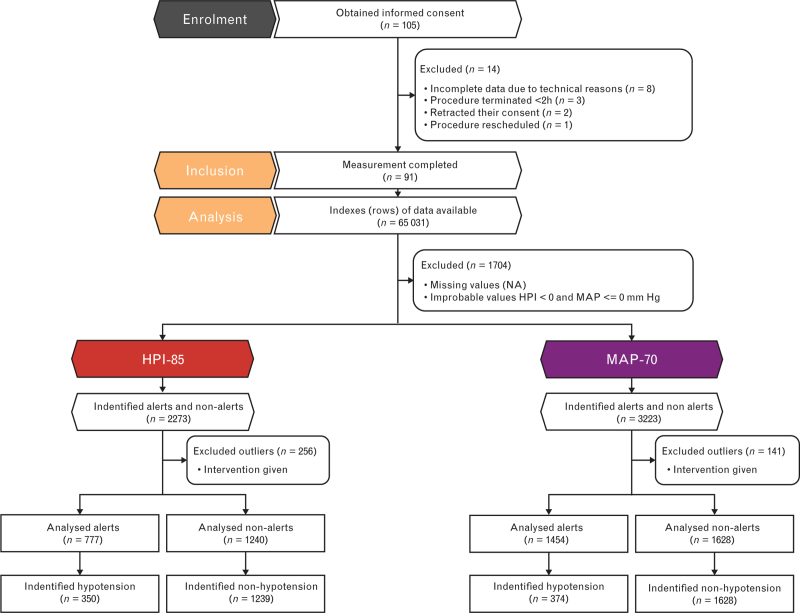
Participants: Adults scheduled for elective non-cardiac surgery lasting over two hours. Of the 105 eligible patients, 91 had sufficient data for analysis.
Main outcome measures: The primary outcome was the time-to-hypotensive event intervals predicted by HPI popup alerts (≥85 for ≥40 s) and MAP-alerts (70-75 mmHg). Secondary analyses examined differences between these predictors regarding the PPV and missed event rates, as well as the difference in these metrics between instant HPI-85 alerts and the six MAP-alerts.
Results: The largest time-to-event difference was seen between HPI-85 popup and MAP-70 alerts, with a gain of 0.58 (95% confidence interval (CI), 0.57 to 0.58) min, favouring HPI. Higher MAP thresholds reduced this time difference, but worsened PPV values, with 20.5 (95% CI, 20.3 to 20.6)% at MAP-75 compared to 55.6 (95% CI, 55.4 to 55.8)% for HPI-85 popups. Missed event proportions were similar: between one to three percent. Instant HPI-85 and MAP-72 alerts showed comparable performance, but both had suboptimal PPV values around 30%. However, adding a 40-s time-dependence to MAP's alert definition levelled the differences across the three evaluated metrics, aligning more closely with HPI-85 popup alerts.
Conclusions: Using HPI-85 popup alerts does not provide additional prediction time over MAP-alerts in the 70 to 75 mmHg range, but they may be preferred due to higher PPV values. Instant HPI-85 and MAP-alerts perform similarly, with MAP-72 being closest, though these alerts more frequently occur regardless of subsequent hypotension with the potential to introduce unnecessary treatment. Adding a 40-s time-dependence to MAP-alerts to match the HPI popup characteristic eliminates distinctions between prediction time and missed events, while maintaining the higher PPV. However, whether 40sec-MAP-alerts are clinically equivalent remains to be determined in prospective clinical trials.
Trial registration: Clinicaltrials.gov NCT03795831 on 10 January 2019.
期刊介绍:
The European Journal of Anaesthesiology (EJA) publishes original work of high scientific quality in the field of anaesthesiology, pain, emergency medicine and intensive care. Preference is given to experimental work or clinical observation in man, and to laboratory work of clinical relevance. The journal also publishes commissioned reviews by an authority, editorials, invited commentaries, special articles, pro and con debates, and short reports (correspondences, case reports, short reports of clinical studies).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


