Olivia Duru, Ryan G Eaton, Nathan Ritchey, Sharon Heaton, Ciarán J Powers
{"title":"Racial and gender disparities in patients undergoing mechanical thrombectomy for large vessel occlusion at a comprehensive stroke center.","authors":"Olivia Duru, Ryan G Eaton, Nathan Ritchey, Sharon Heaton, Ciarán J Powers","doi":"10.4103/bc.bc_66_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Mechanical thrombectomy (MT) is the standard of care for acute ischemic stroke for select patients with large vessel occlusion (LVO). Although racial disparities in the utilization of thrombectomy have been previously identified, disparities in the utilization of thrombectomy in a single center with a standardized patient selection protocol have not been described in the literature.</p><p><strong>Methods: </strong>Using the American Heart Association Quality Improvement Programs Registry, we retrospectively reviewed the records of 1,143 patients with LVO between December 1, 2014, and May 31, 2021. Patient records were assessed for demographic data, stroke risk factors, process metrics, and success of thrombectomy. A Pearson's Chi-Squared and an independent two-sample <i>t</i>-test were used to determine the significance. Following this, a multivariate logistic regression was run to determine predictably of thrombectomy outcomes.</p><p><strong>Results: </strong>Of the 1,143 LVO patients, 567 were male (49.6%), 576 were female, (50.4%), 963 were white (84.3%), and 180 were nonwhite (15.7%). Based on our Pearson's Chi-squared analysis, female patients were more like to undergo thrombectomy compared to male patients (62.4% vs. 48.9%; <i>P</i> < 0.001). White patients were also more likely to undergo thrombectomy compared to nonwhite patients (58.7% vs. 39.7%; <i>P</i> < 0.001). After the multivariate logistic regression analysis and after controlling for comorbidities, insurance status, age, time to presentation (last known well to arrival), transfer from outside hospital, and zip codes, white patients were 2.29 times more likely to receive a thrombectomy compared to nonwhite patients (odds ratio [OR], 2.29, 95% confidence interval [CI], 1.33, 3.944). Patients with Medicare insurance were 33.57 times more likely to receive a thrombectomy compared to those without medicare (OR, 33.57, 95% CI, 20.37, 55.327). In the regression model, sex did not contribute significantly to the likelihood of receiving a thrombectomy.</p><p><strong>Conclusions: </strong>White patients were more likely to undergo MT. Female patients tended to have higher rates of MT, accounting for the fact that other variables could have influenced this. These disparities may result from a multitude of other factors such as eligibility for MT, delayed presentation, and adequate diagnosis of LVO in the emergency department. This study highlights the importance of and potential causes of these disparities. Further investigation with data from multiple centers is necessary to validate these findings and identify strategies for improving utilization of thrombectomy.</p>","PeriodicalId":9288,"journal":{"name":"Brain Circulation","volume":"10 4","pages":"330-335"},"PeriodicalIF":4.8000,"publicationDate":"2024-12-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11850938/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain Circulation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4103/bc.bc_66_24","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Mechanical thrombectomy (MT) is the standard of care for acute ischemic stroke for select patients with large vessel occlusion (LVO). Although racial disparities in the utilization of thrombectomy have been previously identified, disparities in the utilization of thrombectomy in a single center with a standardized patient selection protocol have not been described in the literature.
Methods: Using the American Heart Association Quality Improvement Programs Registry, we retrospectively reviewed the records of 1,143 patients with LVO between December 1, 2014, and May 31, 2021. Patient records were assessed for demographic data, stroke risk factors, process metrics, and success of thrombectomy. A Pearson's Chi-Squared and an independent two-sample t-test were used to determine the significance. Following this, a multivariate logistic regression was run to determine predictably of thrombectomy outcomes.
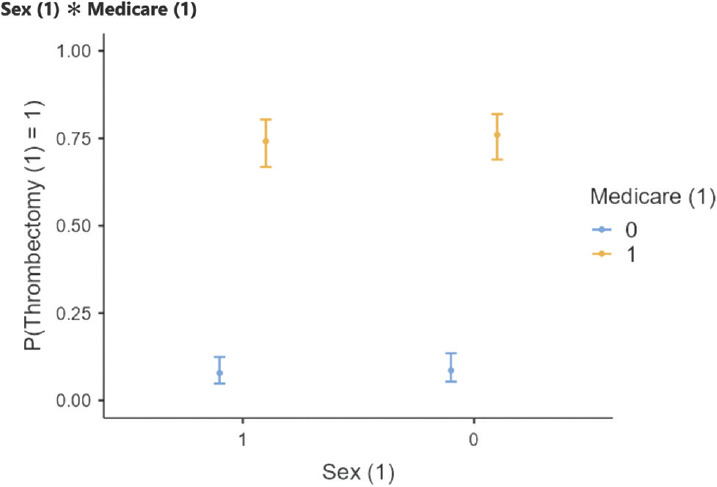
Results: Of the 1,143 LVO patients, 567 were male (49.6%), 576 were female, (50.4%), 963 were white (84.3%), and 180 were nonwhite (15.7%). Based on our Pearson's Chi-squared analysis, female patients were more like to undergo thrombectomy compared to male patients (62.4% vs. 48.9%; P < 0.001). White patients were also more likely to undergo thrombectomy compared to nonwhite patients (58.7% vs. 39.7%; P < 0.001). After the multivariate logistic regression analysis and after controlling for comorbidities, insurance status, age, time to presentation (last known well to arrival), transfer from outside hospital, and zip codes, white patients were 2.29 times more likely to receive a thrombectomy compared to nonwhite patients (odds ratio [OR], 2.29, 95% confidence interval [CI], 1.33, 3.944). Patients with Medicare insurance were 33.57 times more likely to receive a thrombectomy compared to those without medicare (OR, 33.57, 95% CI, 20.37, 55.327). In the regression model, sex did not contribute significantly to the likelihood of receiving a thrombectomy.
Conclusions: White patients were more likely to undergo MT. Female patients tended to have higher rates of MT, accounting for the fact that other variables could have influenced this. These disparities may result from a multitude of other factors such as eligibility for MT, delayed presentation, and adequate diagnosis of LVO in the emergency department. This study highlights the importance of and potential causes of these disparities. Further investigation with data from multiple centers is necessary to validate these findings and identify strategies for improving utilization of thrombectomy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


