How I Investigate Measurable Residual Disease in B-Cell Precursor Acute Lymphoblastic Leukemia After Therapy With Bi-Specific Monoclonal Antibodies and 19CAR-T Cells
Maura Rosane Valerio Ikoma-Colturato, Felipe Magalhães Furtado, Elen de Oliveira, Fabiola Gevert, Roberia Mendonça, The Brazilian Society of Bone Marrow and Cell Therapy (SBTMO) MRD Working Group
{"title":"How I Investigate Measurable Residual Disease in B-Cell Precursor Acute Lymphoblastic Leukemia After Therapy With Bi-Specific Monoclonal Antibodies and 19CAR-T Cells","authors":"Maura Rosane Valerio Ikoma-Colturato, Felipe Magalhães Furtado, Elen de Oliveira, Fabiola Gevert, Roberia Mendonça, The Brazilian Society of Bone Marrow and Cell Therapy (SBTMO) MRD Working Group","doi":"10.1111/ijlh.14448","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>Measurable residual disease (MRD) in B-cell precursor acute lymphoblastic leukemia (BCP-ALL) following anti-CD19 targeted therapies requires specific strategies to identify residual blast cells due to loss or reduced CD19 expression that makes it inconsistent as a primitive marker for B-cell gating.</p>\n </section>\n \n <section>\n \n <h3> Objective</h3>\n \n <p>Due to the increased access of BCP-ALL patients to therapies with CD3/CD19 bispecific T-cell engagers (BiTe) and CD19-targeted chimeric antigen receptor T-Cell (CAR-T), it is essential that flow cytometry laboratories are prepared to evaluate therapeutic responses.</p>\n </section>\n \n <section>\n \n <h3> Material and Methods</h3>\n \n <p>Here, validated strategies for MRD detection in the context of anti-CD19 therapies are described, accessible to flow cytometry laboratories according to their different facilities. The paper includes an 8-color flow cytometry (FC) strategy for BCP-ALL MRD based on alternative gating without the use of additional markers (Euroflow protocol), as well as other strategies using alternative markers to CD19, comprising 2 protocols using 8 colors, one using 10 colors and another 14 colors/15 markers.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Different strategies are needed to detect MRD without using CD19 for B-cell population gating after CD19-targeted therapies. However, it is essential that validated protocols are used according to the available resources to ensure reliable results for clinical decision-making.</p>\n </section>\n </div>","PeriodicalId":14120,"journal":{"name":"International Journal of Laboratory Hematology","volume":"47 3","pages":"398-406"},"PeriodicalIF":2.3000,"publicationDate":"2025-02-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ijlh.14448","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Laboratory Hematology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ijlh.14448","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction
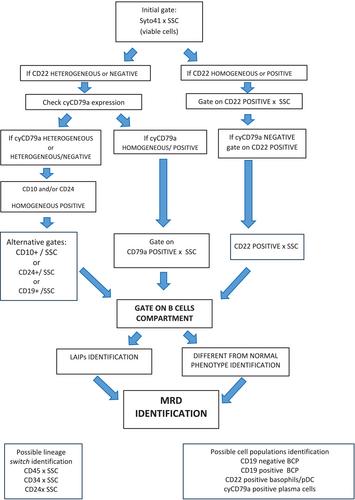
Measurable residual disease (MRD) in B-cell precursor acute lymphoblastic leukemia (BCP-ALL) following anti-CD19 targeted therapies requires specific strategies to identify residual blast cells due to loss or reduced CD19 expression that makes it inconsistent as a primitive marker for B-cell gating.
Objective
Due to the increased access of BCP-ALL patients to therapies with CD3/CD19 bispecific T-cell engagers (BiTe) and CD19-targeted chimeric antigen receptor T-Cell (CAR-T), it is essential that flow cytometry laboratories are prepared to evaluate therapeutic responses.
Material and Methods
Here, validated strategies for MRD detection in the context of anti-CD19 therapies are described, accessible to flow cytometry laboratories according to their different facilities. The paper includes an 8-color flow cytometry (FC) strategy for BCP-ALL MRD based on alternative gating without the use of additional markers (Euroflow protocol), as well as other strategies using alternative markers to CD19, comprising 2 protocols using 8 colors, one using 10 colors and another 14 colors/15 markers.
Conclusion
Different strategies are needed to detect MRD without using CD19 for B-cell population gating after CD19-targeted therapies. However, it is essential that validated protocols are used according to the available resources to ensure reliable results for clinical decision-making.
期刊介绍:
The International Journal of Laboratory Hematology provides a forum for the communication of new developments, research topics and the practice of laboratory haematology.
The journal publishes invited reviews, full length original articles, and correspondence.
The International Journal of Laboratory Hematology is the official journal of the International Society for Laboratory Hematology, which addresses the following sub-disciplines: cellular analysis, flow cytometry, haemostasis and thrombosis, molecular diagnostics, haematology informatics, haemoglobinopathies, point of care testing, standards and guidelines.
The journal was launched in 2006 as the successor to Clinical and Laboratory Hematology, which was first published in 1979. An active and positive editorial policy ensures that work of a high scientific standard is reported, in order to bridge the gap between practical and academic aspects of laboratory haematology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


