Feasibility and safety of robotic radical resection for hilar cholangiocarcinoma in highly selected patients: A systematic review and meta-analysis with meta-regression.
Shahab Hajibandeh, Shahin Hajibandeh, Thomas Satyadas
{"title":"Feasibility and safety of robotic radical resection for hilar cholangiocarcinoma in highly selected patients: A systematic review and meta-analysis with meta-regression.","authors":"Shahab Hajibandeh, Shahin Hajibandeh, Thomas Satyadas","doi":"10.14701/ahbps.24-236","DOIUrl":null,"url":null,"abstract":"<p><p>To examine the feasibility and safety of robotic radical resection (RRR) for hilar cholangiocarcinoma (HCCA). A PRISMA-compliant meta-analysis with meta-regression was conducted, including studies reporting outcomes of RRR in patients with HCCA. Six studies comprising 295 patients were included. In highly selected patients (body mass index [BMI] < 25 kg/m\" ; tumor size < 3 cm), RRR of HCCA proved safe and feasible (Clavien-Dindo ≥ III complications: 14.8% [95% confidence interval 8.7%-20.8%]; 30-day mortality: 1.9% [0%-4.2%]; conversion to open surgery: 1.9% [0%-4.2%]; intraoperative blood loss: 210 mL [119-301 mL]; operative time: 481 minutes [339-623 minutes]; R0 resection rate: 82.2% [75.0%-89.4%]; retrieved lymph nodes: 12 [9-16]). Younger age (<i>p</i> = 0.008), higher BMI (<i>p</i> = 0.009), larger tumors (<i>p</i> = 0.048), and performing liver resections (<i>p</i> = 0.017) increased blood loss. American Society of Anesthesiologists status ≥ III (<i>p</i> < 0.001) and Bismuth IV disease (<i>p</i> < 0.001) increased operative times. Preoperative biliary drainage (<i>p</i> = 0.027) enhanced R0 resection rates. RRR led to less bleeding (mean difference [MD]: -184 mL, <i>p</i> = 0.0005), longer operative times (MD: 162 minutes, <i>p</i> = 0.001), and improved R0 resection rates (odds ratio: 3.29, <i>p</i> = 0.006) compared with the open approach. Subject to selection bias and type 2 error, RRR for HCCA might be safe and feasible in highly selected patients (favorable BMI and tumor size). The findings should not be taken as definitive conclusions but may be used for hypothesis generation in subsequent trials.</p>","PeriodicalId":72220,"journal":{"name":"Annals of hepato-biliary-pancreatic surgery","volume":" ","pages":"99-112"},"PeriodicalIF":1.7000,"publicationDate":"2025-05-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12093240/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of hepato-biliary-pancreatic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14701/ahbps.24-236","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/26 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
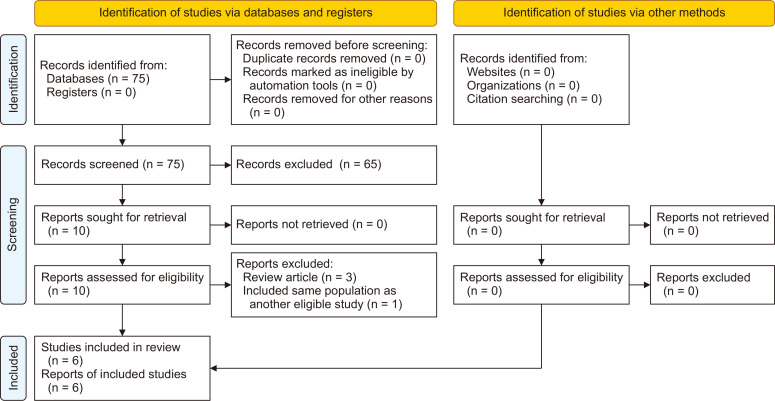
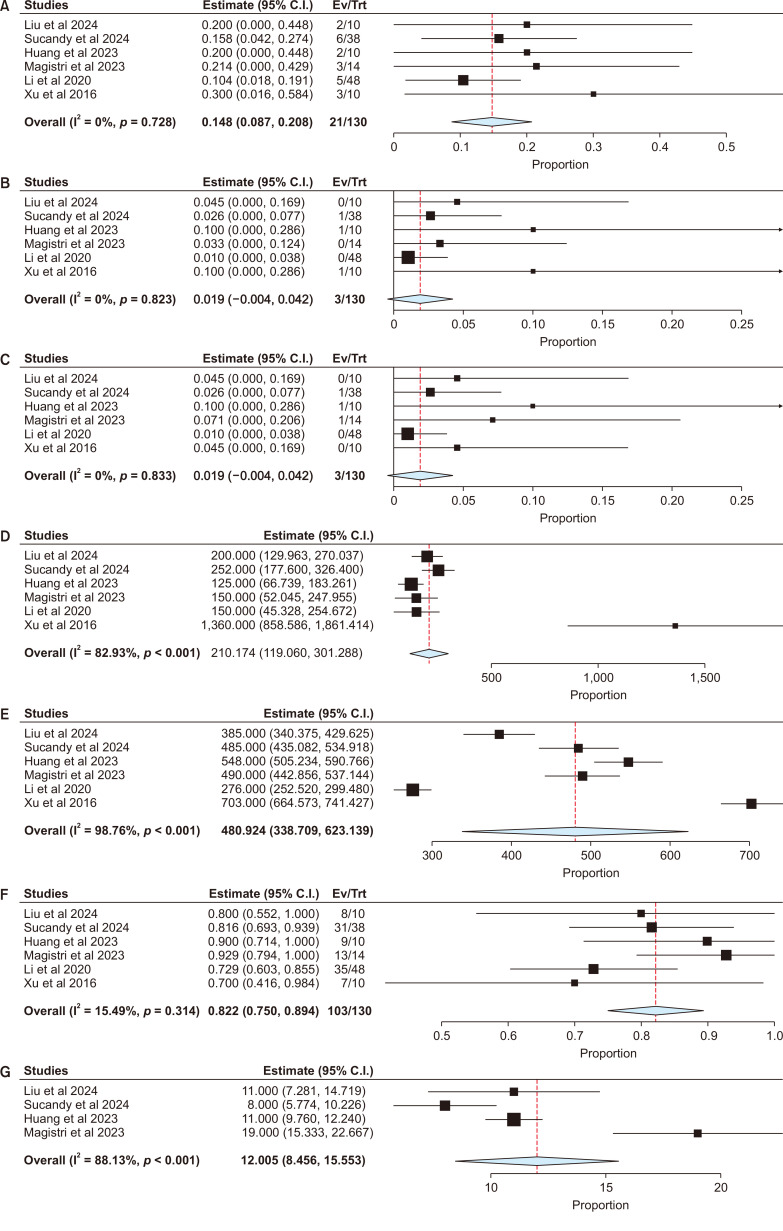
To examine the feasibility and safety of robotic radical resection (RRR) for hilar cholangiocarcinoma (HCCA). A PRISMA-compliant meta-analysis with meta-regression was conducted, including studies reporting outcomes of RRR in patients with HCCA. Six studies comprising 295 patients were included. In highly selected patients (body mass index [BMI] < 25 kg/m" ; tumor size < 3 cm), RRR of HCCA proved safe and feasible (Clavien-Dindo ≥ III complications: 14.8% [95% confidence interval 8.7%-20.8%]; 30-day mortality: 1.9% [0%-4.2%]; conversion to open surgery: 1.9% [0%-4.2%]; intraoperative blood loss: 210 mL [119-301 mL]; operative time: 481 minutes [339-623 minutes]; R0 resection rate: 82.2% [75.0%-89.4%]; retrieved lymph nodes: 12 [9-16]). Younger age (p = 0.008), higher BMI (p = 0.009), larger tumors (p = 0.048), and performing liver resections (p = 0.017) increased blood loss. American Society of Anesthesiologists status ≥ III (p < 0.001) and Bismuth IV disease (p < 0.001) increased operative times. Preoperative biliary drainage (p = 0.027) enhanced R0 resection rates. RRR led to less bleeding (mean difference [MD]: -184 mL, p = 0.0005), longer operative times (MD: 162 minutes, p = 0.001), and improved R0 resection rates (odds ratio: 3.29, p = 0.006) compared with the open approach. Subject to selection bias and type 2 error, RRR for HCCA might be safe and feasible in highly selected patients (favorable BMI and tumor size). The findings should not be taken as definitive conclusions but may be used for hypothesis generation in subsequent trials.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


