{"title":"An Intra-Abdominal Desmoid Tumor with Edematous Loose Collagen Fibers.","authors":"Mao Iino, Shoji Oura","doi":"10.1159/000543498","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Diagnostic physicians tend to judge a low-dense area on computed tomography (CT) as central necrosis when it has no contrast enhancement and locates in the center of large tumors.</p><p><strong>Case presentation: </strong>An 80-year-old woman was referred to our hospital due to the detection of an abdominal mass on ultrasound (US). CT showed a well-demarcated oval mass, 11 cm in size, with a central low-density area. US showed high internal echoes and enhanced posterior echoes. Magnetic resonance imaging (MRI) showed the low-density area on CT to be hypo-intense on T1-weighted images and hyper-intense on T2-weighted images. MRI further showed the central part of the tumor to be hyper-intense both on diffusion-weighted images and apparent diffusion coefficient images. Under the tentative diagnosis of a gastrointestinal stromal tumor with central necrosis, the patient underwent tumor resection, revealing the tumor to be a jejunal submucosal tumor. Pathological study showed collagen fibers with heterogeneous density and sparse proliferation of spindle cells. The center of the tumor had marked edema in addition to sparse collagen fibers. Immunostaining showed that the atypical cells were diffusely positive for β catenin and negative for S100 protein, desmin, and DOG1, leading to the diagnosis of desmoid tumor (DT).</p><p><strong>Conclusions: </strong>Physicians should note that intra-abdominal DT can have edematous loose collagen fibers and may show central necrosis-like findings on CT.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"19 1","pages":"107-112"},"PeriodicalIF":0.6000,"publicationDate":"2025-02-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11857155/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000543498","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Diagnostic physicians tend to judge a low-dense area on computed tomography (CT) as central necrosis when it has no contrast enhancement and locates in the center of large tumors.
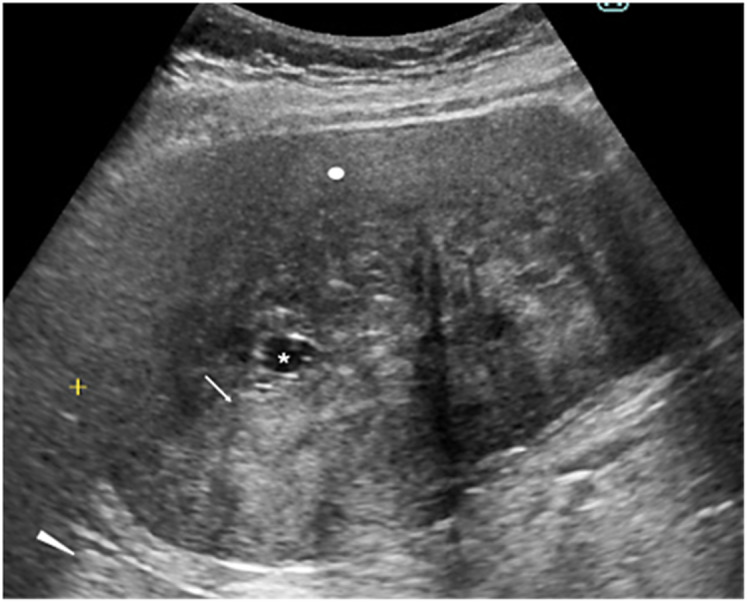
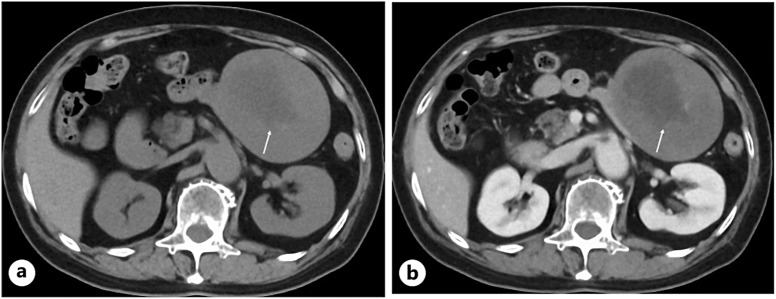
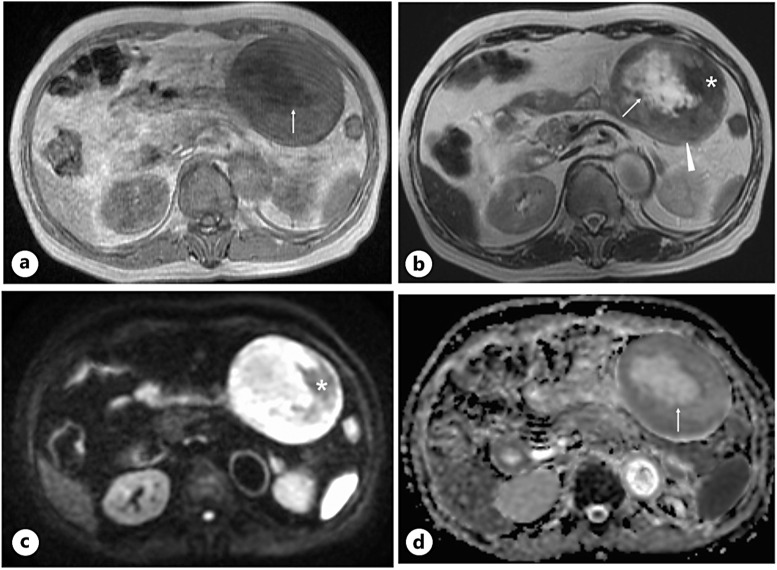
Case presentation: An 80-year-old woman was referred to our hospital due to the detection of an abdominal mass on ultrasound (US). CT showed a well-demarcated oval mass, 11 cm in size, with a central low-density area. US showed high internal echoes and enhanced posterior echoes. Magnetic resonance imaging (MRI) showed the low-density area on CT to be hypo-intense on T1-weighted images and hyper-intense on T2-weighted images. MRI further showed the central part of the tumor to be hyper-intense both on diffusion-weighted images and apparent diffusion coefficient images. Under the tentative diagnosis of a gastrointestinal stromal tumor with central necrosis, the patient underwent tumor resection, revealing the tumor to be a jejunal submucosal tumor. Pathological study showed collagen fibers with heterogeneous density and sparse proliferation of spindle cells. The center of the tumor had marked edema in addition to sparse collagen fibers. Immunostaining showed that the atypical cells were diffusely positive for β catenin and negative for S100 protein, desmin, and DOG1, leading to the diagnosis of desmoid tumor (DT).
Conclusions: Physicians should note that intra-abdominal DT can have edematous loose collagen fibers and may show central necrosis-like findings on CT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


