{"title":"Spontaneous Regression of Advanced Transverse Colon Cancer: A Case Report.","authors":"Shinya Ohno, Yoshinori Iwata, Saki Mitsutome, Shusaku Kawai, Manabu Neo, Moe Fukuda, Bei Wang, Tomonari Suetsugu, Taku Watanabe, Shuji Komori, Chihiro Tanaka, Narutoshi Nagao, Masahiko Kawai","doi":"10.70352/scrj.cr.24-0018","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The incidence of spontaneous regression (SR) of malignancy is one in 60000-100000 cancer patients and spontaneous regression in colorectal cancer is quite rare, reported to account for less than 2% of spontaneous regression of malignancy. In recent years, some reports of spontaneous regression in colorectal cancer in patients with high-frequency microsatellite instability have suggested a deep association between high-frequency microsatellite instability and spontaneous regression. We report our experience of spontaneous regression of advanced colorectal cancer with high-frequency microsatellite instability and provide a review of spontaneous regression in colorectal cancer.</p><p><strong>Case presentation: </strong>An 83-year-old woman was diagnosed as having advanced colorectal cancer in the transverse colon by lower gastrointestinal endoscopy, and biopsy results revealed moderately differentiated adenocarcinoma. Contrast-enhanced computed tomography showed a tumor located near the hepatic flexure and an enlarged lymph node near the tumor. No distant metastasis was observed, and the preoperative diagnosis was cT3N1aM0 cStage IIIb cancer. Immunohistochemical analysis of the biopsy specimen suggested deficient mismatch repair. During the wait for surgery, the patient was urgently hospitalized due to severe dehydration. After her general condition improved, 38 days after the biopsy, we performed laparoscopic resection of the partial ascending and transverse colon with D3 lymph node dissection. The tumor noted preoperatively was not present in the specimen, and intraoperative endoscopy revealed no tumor on the anorectal side. Additional ileocecal resection was performed, but no tumor was found in the specimen, and another intraoperative endoscopy was performed, which revealed a discolored scar near the anal margin. We determined that tumor loss or morphological change had occurred, so after additional resection of the same area, ultimately, an extended right hemicolectomy was performed. Histopathological diagnosis was pT0N0M0 pStage0 cancer with no residual tumor. The patient has progressed without recurrence at 1 year after the operation.</p><p><strong>Conclusions: </strong>The immunological response due to high-frequency microsatellite instability may be related to the mechanism of spontaneous regression in colorectal cancer. If high-frequency microsatellite instability is diagnosed preoperatively, we recommend that the tumor location should be confirmed preoperatively.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"11 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11842877/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.70352/scrj.cr.24-0018","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/31 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The incidence of spontaneous regression (SR) of malignancy is one in 60000-100000 cancer patients and spontaneous regression in colorectal cancer is quite rare, reported to account for less than 2% of spontaneous regression of malignancy. In recent years, some reports of spontaneous regression in colorectal cancer in patients with high-frequency microsatellite instability have suggested a deep association between high-frequency microsatellite instability and spontaneous regression. We report our experience of spontaneous regression of advanced colorectal cancer with high-frequency microsatellite instability and provide a review of spontaneous regression in colorectal cancer.
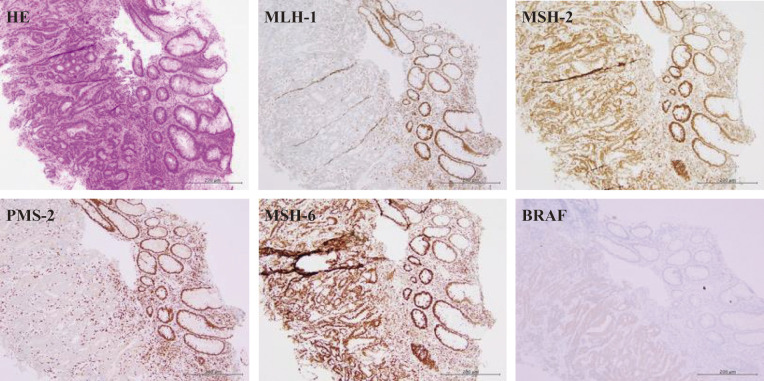
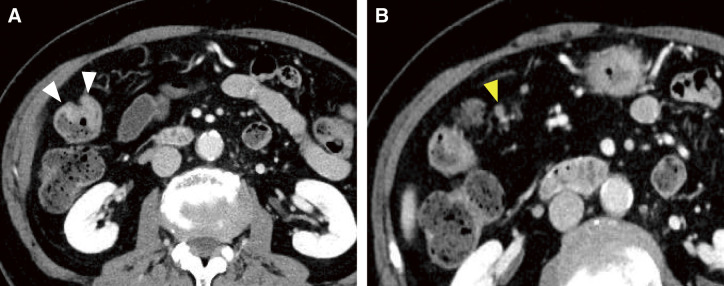
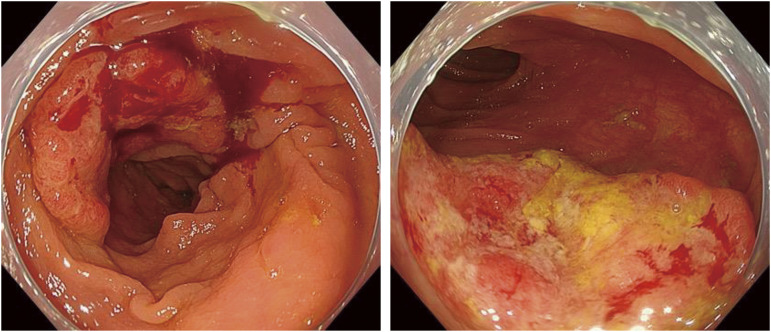
Case presentation: An 83-year-old woman was diagnosed as having advanced colorectal cancer in the transverse colon by lower gastrointestinal endoscopy, and biopsy results revealed moderately differentiated adenocarcinoma. Contrast-enhanced computed tomography showed a tumor located near the hepatic flexure and an enlarged lymph node near the tumor. No distant metastasis was observed, and the preoperative diagnosis was cT3N1aM0 cStage IIIb cancer. Immunohistochemical analysis of the biopsy specimen suggested deficient mismatch repair. During the wait for surgery, the patient was urgently hospitalized due to severe dehydration. After her general condition improved, 38 days after the biopsy, we performed laparoscopic resection of the partial ascending and transverse colon with D3 lymph node dissection. The tumor noted preoperatively was not present in the specimen, and intraoperative endoscopy revealed no tumor on the anorectal side. Additional ileocecal resection was performed, but no tumor was found in the specimen, and another intraoperative endoscopy was performed, which revealed a discolored scar near the anal margin. We determined that tumor loss or morphological change had occurred, so after additional resection of the same area, ultimately, an extended right hemicolectomy was performed. Histopathological diagnosis was pT0N0M0 pStage0 cancer with no residual tumor. The patient has progressed without recurrence at 1 year after the operation.
Conclusions: The immunological response due to high-frequency microsatellite instability may be related to the mechanism of spontaneous regression in colorectal cancer. If high-frequency microsatellite instability is diagnosed preoperatively, we recommend that the tumor location should be confirmed preoperatively.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


