Delayed Onset Immune-Related Pituitary Adrenal Insufficiency Induced by Neoadjuvant Nivolumab Therapy for Locally Advanced Lung Cancer in the Postoperative Period: A Case Report.
{"title":"Delayed Onset Immune-Related Pituitary Adrenal Insufficiency Induced by Neoadjuvant Nivolumab Therapy for Locally Advanced Lung Cancer in the Postoperative Period: A Case Report.","authors":"Takafumi Kabuto, Shizuka Kaneko, Shinnosuke Nomura, Satoshi Terashita, Kaito Kitahori, Masaki Ikeda, Naohisa Chiba, Masashi Ishikawa","doi":"10.70352/scrj.cr.24-0044","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Neoadjuvant, adjuvant, and perioperative immune checkpoint inhibitor (ICI) regimens for treating locally advanced lung cancer have dramatically evolved in recent years. Despite these immunotherapies being very promising, they can be associated with potential life-threatening immune-related adverse events (irAEs), and there is not much awareness regarding irAEs in surgical regimens.</p><p><strong>Case presentation: </strong>A Japanese man in his 70s was diagnosed with right upper lobe lung adenocarcinoma (cT3N1[#12u]M0, parietal pleural invasion, cStage IIIA), with the programmed death-ligand 1 expression level of <1%. He underwent right upper lobectomy via open thoracotomy followed by 3 cycles of neoadjuvant cisplatin, pemetrexed, and nivolumab. The pathological response rate was 50% and the pathological stage was ypT2bN0M0, ypStage IIA. Seven months after the surgery, he experienced gradually worsening anorexia, fatigue, and hyponatremia. He was diagnosed with pituitary adrenal insufficiency induced by neoadjuvant immunotherapy by the 100 μg corticotropin-releasing hormone stress test. Cardiogenic shock caused by takotsubo cardiomyopathy occurred, and intensive treatment was performed. Steroid therapy was effective, but the physical dysfunction persisted, although no recurrence of lung cancer was observed.</p><p><strong>Conclusions: </strong>Patients receiving neoadjuvant immunotherapies can develop life-threatening irAEs late in the postoperative period. Surgeons who follow up patients after neoadjuvant immunotherapies must be as vigilant regarding the development of irAEs in the postoperative phase as clinical oncologists.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"11 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11842875/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.70352/scrj.cr.24-0044","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/1 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Neoadjuvant, adjuvant, and perioperative immune checkpoint inhibitor (ICI) regimens for treating locally advanced lung cancer have dramatically evolved in recent years. Despite these immunotherapies being very promising, they can be associated with potential life-threatening immune-related adverse events (irAEs), and there is not much awareness regarding irAEs in surgical regimens.
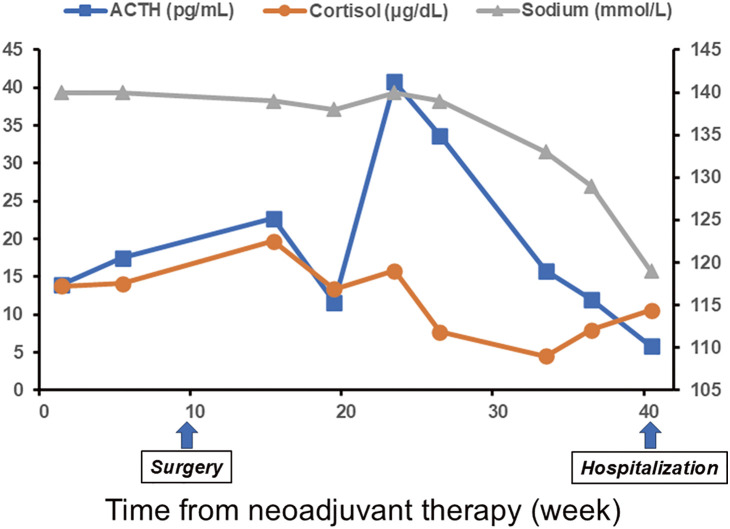
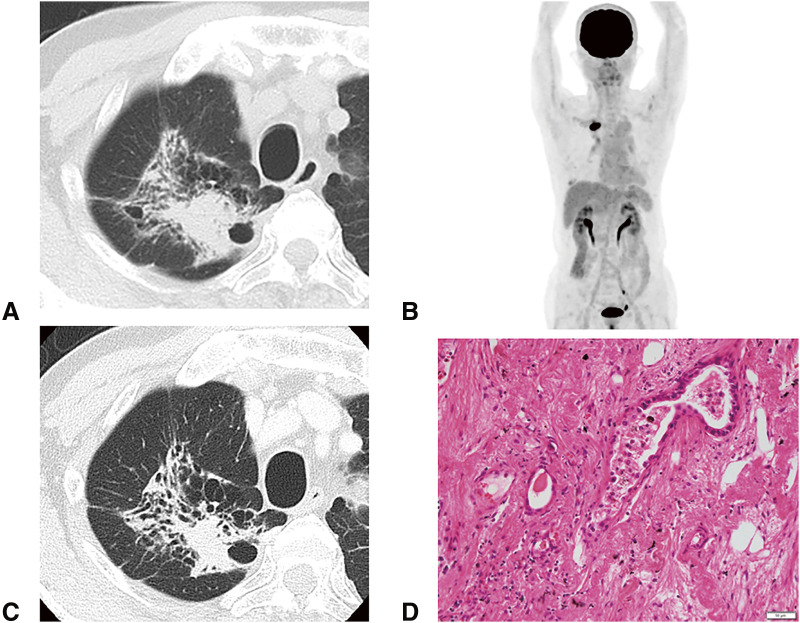
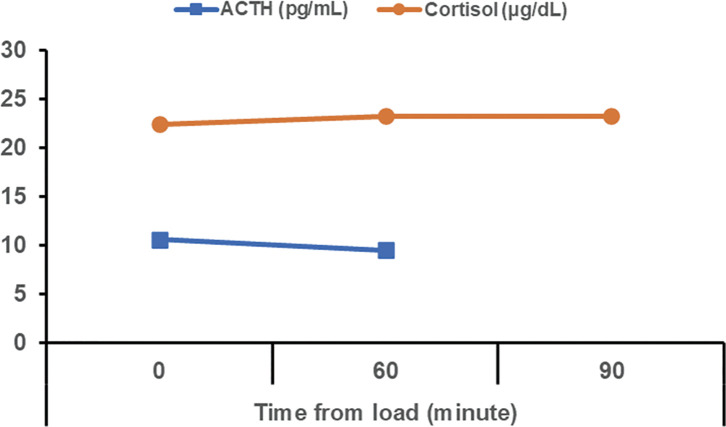
Case presentation: A Japanese man in his 70s was diagnosed with right upper lobe lung adenocarcinoma (cT3N1[#12u]M0, parietal pleural invasion, cStage IIIA), with the programmed death-ligand 1 expression level of <1%. He underwent right upper lobectomy via open thoracotomy followed by 3 cycles of neoadjuvant cisplatin, pemetrexed, and nivolumab. The pathological response rate was 50% and the pathological stage was ypT2bN0M0, ypStage IIA. Seven months after the surgery, he experienced gradually worsening anorexia, fatigue, and hyponatremia. He was diagnosed with pituitary adrenal insufficiency induced by neoadjuvant immunotherapy by the 100 μg corticotropin-releasing hormone stress test. Cardiogenic shock caused by takotsubo cardiomyopathy occurred, and intensive treatment was performed. Steroid therapy was effective, but the physical dysfunction persisted, although no recurrence of lung cancer was observed.
Conclusions: Patients receiving neoadjuvant immunotherapies can develop life-threatening irAEs late in the postoperative period. Surgeons who follow up patients after neoadjuvant immunotherapies must be as vigilant regarding the development of irAEs in the postoperative phase as clinical oncologists.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


