Shirley Sze, Chokanan Thaitirarot, Sunanthiny Krishnan, Daniel Chan, Will Nicolson, Iain Squire, Louise Clayton, Ian Loke
{"title":"Early and rapid initiation of quadruple therapy for heart failure with reduced ejection fraction: A real-world experience.","authors":"Shirley Sze, Chokanan Thaitirarot, Sunanthiny Krishnan, Daniel Chan, Will Nicolson, Iain Squire, Louise Clayton, Ian Loke","doi":"10.1016/j.clinme.2025.100296","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To evaluate the feasibility, safety and efficacy of early and rapid initiation of quadruple therapy (four drugs in 4 weeks - '4×4 approach') for heart failure with reduced ejection fraction (HFrEF) patients in a real-world clinical setting.</p><p><strong>Design: </strong>Prospective service evaluation study.</p><p><strong>Setting: </strong>Secondary care.</p><p><strong>Participants: </strong>Consecutive patients with de novo HFrEF between March and August 2021.</p><p><strong>Intervention: </strong>'4×4 approach' - individualised initiation and up-titration of four pillars of HFrEF therapy by heart failure specialist.</p><p><strong>Main outcome: </strong>Proportion of patients initiated on four pillars of HFrEF therapy within 4 weeks.</p><p><strong>Results: </strong>Of 100 patients approached, 19 patients were not suitable for the rapid initiation and up-titration pathway due to severe frailty and significant comorbidities. 81 patients were enrolled (61% male, median age = 73 years, median N-terminal pro-brain natriuretic peptide [NT-proBNP] = 3,764 ng/L). 39 patients (48%) achieved 4×4. Of the 42 patients who did not, 26 (62%), nine (21%) and seven (17%) patients were on three drugs, two drugs and one drug, respectively. 33 patients had one or more contraindication at the outset; most commonly renal impairment (28%), bradycardia (18%) and hyperkalaemia (15%). Five patients experienced significant side effects during medication up-titration, most commonly symptomatic hypotension. During median follow-up of 554 days, 32 (40%) patients experienced the combined outcome (all-cause hospitalisation/death). Patients who did not achieve 4×4 had an increased risk of the combined outcome (HR 2.25 [1.09-4.68], p=0.029) compared to those who achieved 4×4.</p><p><strong>Conclusion: </strong>Early and rapid initiation of four pillars HFrEF therapy is clinically feasible and safe when implemented in selected patients and is associated with improved clinical outcomes.</p>","PeriodicalId":10492,"journal":{"name":"Clinical Medicine","volume":" ","pages":"100296"},"PeriodicalIF":3.9000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11930596/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.clinme.2025.100296","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/21 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
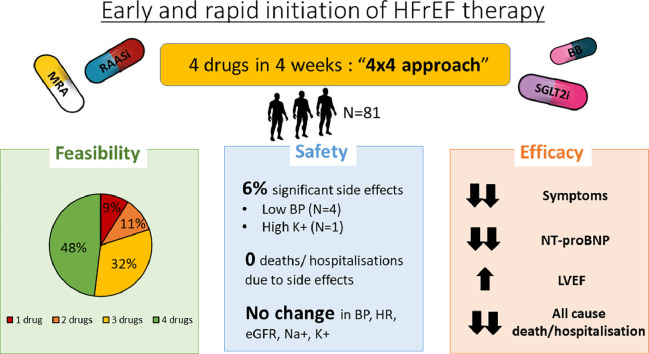
Objectives: To evaluate the feasibility, safety and efficacy of early and rapid initiation of quadruple therapy (four drugs in 4 weeks - '4×4 approach') for heart failure with reduced ejection fraction (HFrEF) patients in a real-world clinical setting.
Design: Prospective service evaluation study.
Setting: Secondary care.
Participants: Consecutive patients with de novo HFrEF between March and August 2021.
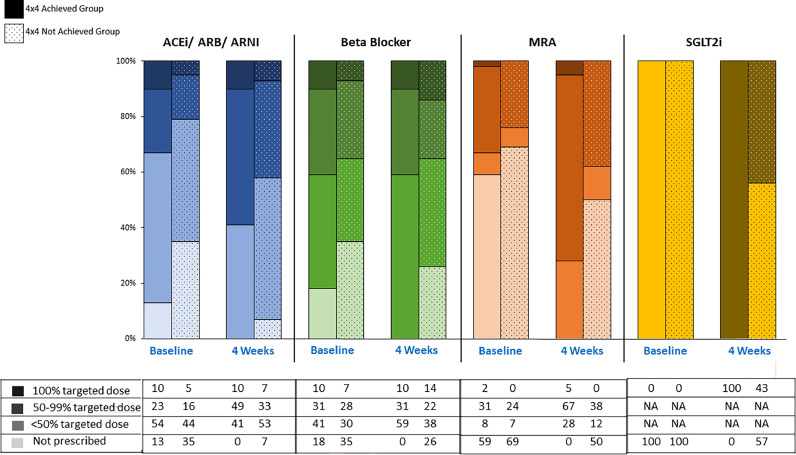
Intervention: '4×4 approach' - individualised initiation and up-titration of four pillars of HFrEF therapy by heart failure specialist.
Main outcome: Proportion of patients initiated on four pillars of HFrEF therapy within 4 weeks.
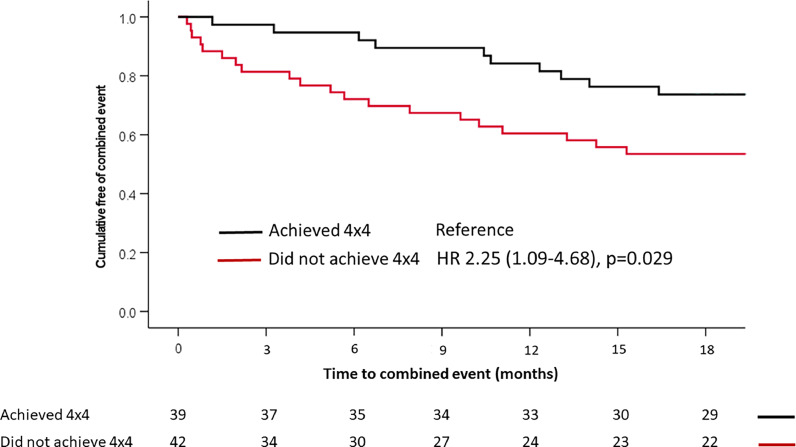
Results: Of 100 patients approached, 19 patients were not suitable for the rapid initiation and up-titration pathway due to severe frailty and significant comorbidities. 81 patients were enrolled (61% male, median age = 73 years, median N-terminal pro-brain natriuretic peptide [NT-proBNP] = 3,764 ng/L). 39 patients (48%) achieved 4×4. Of the 42 patients who did not, 26 (62%), nine (21%) and seven (17%) patients were on three drugs, two drugs and one drug, respectively. 33 patients had one or more contraindication at the outset; most commonly renal impairment (28%), bradycardia (18%) and hyperkalaemia (15%). Five patients experienced significant side effects during medication up-titration, most commonly symptomatic hypotension. During median follow-up of 554 days, 32 (40%) patients experienced the combined outcome (all-cause hospitalisation/death). Patients who did not achieve 4×4 had an increased risk of the combined outcome (HR 2.25 [1.09-4.68], p=0.029) compared to those who achieved 4×4.
Conclusion: Early and rapid initiation of four pillars HFrEF therapy is clinically feasible and safe when implemented in selected patients and is associated with improved clinical outcomes.
期刊介绍:
Clinical Medicine is aimed at practising physicians in the UK and overseas and has relevance to all those managing or working within the healthcare sector.
Available in print and online, the journal seeks to encourage high standards of medical care by promoting good clinical practice through original research, review and comment. The journal also includes a dedicated continuing medical education (CME) section in each issue. This presents the latest advances in a chosen specialty, with self-assessment questions at the end of each topic enabling CPD accreditation to be acquired.
ISSN: 1470-2118 E-ISSN: 1473-4893 Frequency: 6 issues per year

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


