{"title":"Acute Myelin Oligodendrocyte Glycoprotein-IgG Optic Neuritis without Optic Nerve Enhancement.","authors":"Bava Jeyanathan, Jonathan Micieli","doi":"10.1159/000542889","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Optic neuritis (ON) is a common neuro-ophthalmological condition and remains a significant indicator of inflammatory conditions affecting the central nervous system. Varying etiologies exist for ON including multiple sclerosis, NMOSD, and MOGAD. Differential diagnosis is achieved using both radiological and serological testing. MRI characteristics of MOG-ON include T2 hypersensitive lesions, nerve swelling, and gadolinium enhancement of the affected optic nerve. While acute MOG-ON usually presents with optic nerve enhancement, recognizing atypical presentations is critical in accurate diagnosis and effective management.</p><p><strong>Case presentation: </strong>We herein present a case of a 67-year-old woman presenting with sudden decrease in vision in the right eye. The patient underwent a 3T MRI of the orbits and brain 5 days post vision loss which returned normal right optic nerve appearance at presentation (no edema, enhancement or increased T2 signal). Further serological testing of the MOG antibody returned positive (1:100) while APQ4 antibodies were negative. This yielded a diagnosis of MOG-IgG-ON. Subsequently, the patient was treated with IV methylprednisolone 1 g daily for 5 days followed by prednisone 1 mg/kg, resulting in marked improvement in vision.</p><p><strong>Conclusion: </strong>This case highlights the complexity involved in diagnosing ON, especially in the context of MOGAD. Absence of optic nerve enhancement in this patient calls attention to the possibility of subclinical inflammation and/or detectable enhancement later in clinical course. Our findings, along with existing literature, highlight the need for clinicians to consider atypical MRI presentations in MOG-ON cases. Recognizing that normal MRI does not exclude MOG-ON is important for optimizing diagnostic accuracy and effective treatment interventions.</p>","PeriodicalId":9635,"journal":{"name":"Case Reports in Ophthalmology","volume":"16 1","pages":"7-11"},"PeriodicalIF":0.6000,"publicationDate":"2024-12-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11703545/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Ophthalmology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000542889","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"OPHTHALMOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Optic neuritis (ON) is a common neuro-ophthalmological condition and remains a significant indicator of inflammatory conditions affecting the central nervous system. Varying etiologies exist for ON including multiple sclerosis, NMOSD, and MOGAD. Differential diagnosis is achieved using both radiological and serological testing. MRI characteristics of MOG-ON include T2 hypersensitive lesions, nerve swelling, and gadolinium enhancement of the affected optic nerve. While acute MOG-ON usually presents with optic nerve enhancement, recognizing atypical presentations is critical in accurate diagnosis and effective management.
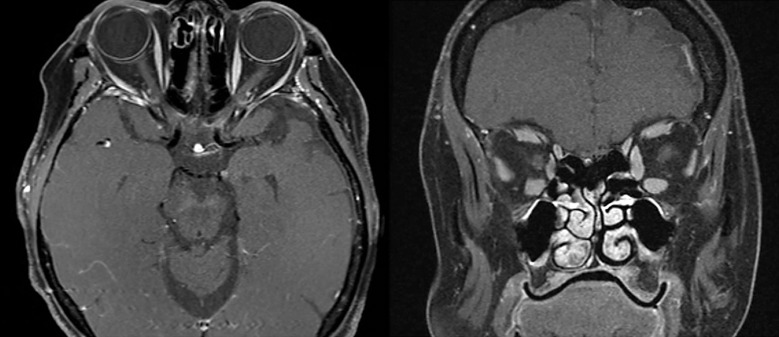
Case presentation: We herein present a case of a 67-year-old woman presenting with sudden decrease in vision in the right eye. The patient underwent a 3T MRI of the orbits and brain 5 days post vision loss which returned normal right optic nerve appearance at presentation (no edema, enhancement or increased T2 signal). Further serological testing of the MOG antibody returned positive (1:100) while APQ4 antibodies were negative. This yielded a diagnosis of MOG-IgG-ON. Subsequently, the patient was treated with IV methylprednisolone 1 g daily for 5 days followed by prednisone 1 mg/kg, resulting in marked improvement in vision.
Conclusion: This case highlights the complexity involved in diagnosing ON, especially in the context of MOGAD. Absence of optic nerve enhancement in this patient calls attention to the possibility of subclinical inflammation and/or detectable enhancement later in clinical course. Our findings, along with existing literature, highlight the need for clinicians to consider atypical MRI presentations in MOG-ON cases. Recognizing that normal MRI does not exclude MOG-ON is important for optimizing diagnostic accuracy and effective treatment interventions.
期刊介绍:
This peer-reviewed online-only journal publishes original case reports covering the entire spectrum of ophthalmology, including prevention, diagnosis, treatment, toxicities of therapy, supportive care, quality-of-life, and survivorship issues. The submission of negative results is strongly encouraged. The journal will also accept case reports dealing with the use of novel technologies, both in the arena of diagnosis and treatment. Supplementary material is welcomed. The intent of the journal is to provide clinicians and researchers with a tool to disseminate their personal experiences to a wider public as well as to review interesting cases encountered by colleagues all over the world. Universally used terms can be searched across the entire growing collection of case reports, further facilitating the retrieval of specific information. Following the open access principle, the entire contents can be retrieved at no charge, guaranteeing easy access to this valuable source of anecdotal information at all times.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


