{"title":"Steroid-Refractory Immune-Related Hepatitis Caused by Pembrolizumab with Stage IVB Non-Small Cell Lung Cancer: A Case Report.","authors":"Tomomi Hamaguchi, Makoto Ueno, Satoshi Kobayashi, Shun Tezuka, Manabu Morimoto, Terufumi Kato, Haruhiro Saito, Shinya Sato, Junji Furuse, Shin Maeda","doi":"10.1159/000542598","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>We report the case of a man in his 50s with stage IVB non-small cell lung cancer who developed severe immune-related hepatitis caused by pembrolizumab.</p><p><strong>Case presentation: </strong>He received carboplatin, pemetrexed, and pembrolizumab as first-line therapy. After four courses, each of the triplet regimen and maintenance therapy with pemetrexed and pembrolizumab, the patient developed immune-related pneumonitis and colitis. Therefore, pemetrexed and pembrolizumab were discontinued, and 0.5 mg/kg/day prednisolone was started. Despite gradual reduction of the prednisolone to 15 mg/day along with resolution of the pneumonitis and colitis, hepatic dysfunction occurred (elevated serum bilirubin and transaminase levels). We made a diagnosis of immune-related hepatitis based on liver biopsy results and negative results for other causes, such as viral infection. We increased the prednisolone dose to 2 mg/kg/day; however, the hepatic dysfunction was not resolved. Upon sequential methylprednisolone pulse therapy (1,000 mg/day), mycophenolate mofetil, and azathioprine treatment, the hepatic dysfunction plateaued but was not resolved. The patient did not respond to steroids for immune-related hepatitis, developed infectious enteritis owing to a compromised state, and died of sepsis on day 107 after diagnosis of immune-related hepatitis.</p><p><strong>Conclusion: </strong>This case highlights the importance of early diagnosis of steroid-refractory disease, prompt initiation of immunosuppressive agents, and steroid dose reduction in such cases. The changes in liver function during steroid non-response and immunosuppressive drug induction in this case are valuable as a reference for future cases of immune-related adverse event hepatitis.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"19 1","pages":"14-21"},"PeriodicalIF":0.6000,"publicationDate":"2024-12-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11666266/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000542598","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: We report the case of a man in his 50s with stage IVB non-small cell lung cancer who developed severe immune-related hepatitis caused by pembrolizumab.
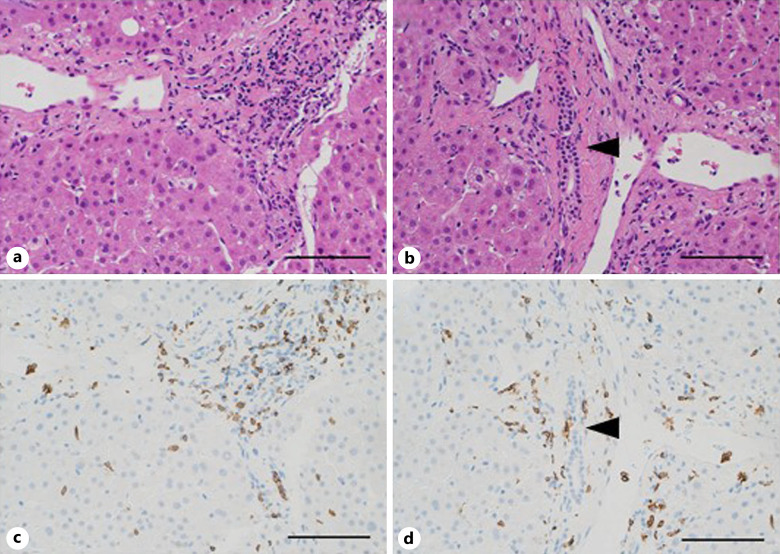
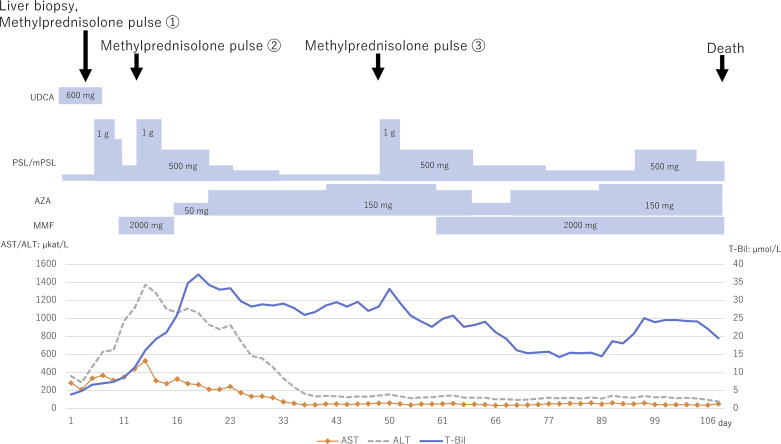
Case presentation: He received carboplatin, pemetrexed, and pembrolizumab as first-line therapy. After four courses, each of the triplet regimen and maintenance therapy with pemetrexed and pembrolizumab, the patient developed immune-related pneumonitis and colitis. Therefore, pemetrexed and pembrolizumab were discontinued, and 0.5 mg/kg/day prednisolone was started. Despite gradual reduction of the prednisolone to 15 mg/day along with resolution of the pneumonitis and colitis, hepatic dysfunction occurred (elevated serum bilirubin and transaminase levels). We made a diagnosis of immune-related hepatitis based on liver biopsy results and negative results for other causes, such as viral infection. We increased the prednisolone dose to 2 mg/kg/day; however, the hepatic dysfunction was not resolved. Upon sequential methylprednisolone pulse therapy (1,000 mg/day), mycophenolate mofetil, and azathioprine treatment, the hepatic dysfunction plateaued but was not resolved. The patient did not respond to steroids for immune-related hepatitis, developed infectious enteritis owing to a compromised state, and died of sepsis on day 107 after diagnosis of immune-related hepatitis.
Conclusion: This case highlights the importance of early diagnosis of steroid-refractory disease, prompt initiation of immunosuppressive agents, and steroid dose reduction in such cases. The changes in liver function during steroid non-response and immunosuppressive drug induction in this case are valuable as a reference for future cases of immune-related adverse event hepatitis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


