{"title":"Fasciitis-panniculitis syndrome with autoantibodies reacting to adipocyte pericellular fibers: a case report.","authors":"Yu Uehara, Takuji Enya, Kohei Miyazaki, Yoshiyuki Hakata, Sachiyo Kawahara, Masaaki Miyazawa, Keisuke Sugimoto","doi":"10.1186/s12969-025-01071-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Fasciitis-panniculitis syndrome (FPS) typically presents with swelling and skin hardening. Its histopathological characteristics include inflammatory cell infiltration and fibrous thickening of the subcutaneous tissue and fascia. Panniculitides in children are rare and only a small number of juvenile FPS cases have been reported. We encountered a case of a 10-year-old boy in which autoantibodies reactive to adipocyte pericellular fibers were detected in relapsing FPS.</p><p><strong>Case presentation: </strong>The patient developed a high fever and skin swelling with pain and erythema on the right side of his body following an abrasion injury on his right wrist at the age of 5 years, and was suspected of having streptococcal toxic shock-like syndrome, for which he received antimicrobials, immunoglobulin therapy, debridement, and plasma exchange. The same manifestations with similar magnetic resonance imaging (MRI) findings of high signal on short tau inversion recovery showing the spread of inflammation in the fat tissue and fascia was observed twice at the age of 6 years. Serological analyses for conventional autoantibodies, bone marrow aspiration, and whole-exome sequencing examination were non-remarkable. Prednisolone was effective in ameliorating the above putative autoinflammatory syndrome. The patient was admitted at the age of 10 years with similar clinical and MRI findings indicative of recurrence of the same disease. En bloc biopsy from the skin to the fascia showed thickening of collagen fibers, infiltration of inflammatory cells composed mainly of neutrophils and lymphocytes, and necrotizing vasculitis in the fat tissue and fascia. Immunohistochemical staining of the en bloc biopsy sections indicated infiltration of T lymphocytes and macrophages in the perivascular connective tissue and fibrinoid necrosis, supporting the diagnosis of FPS. Induction therapy with prednisolone resulted in a remission. IgG purified from the patient's serum reacted with pericellular basement membranes in the subcutaneous fat tissue by immunohistochemistry. The patient is currently taking famotidine to prevent relapses and is making good progress in his recovery.</p><p><strong>Conclusions: </strong>Although pathogenic autoantibodies have not been described in FPS, our results suggest that fat-tissue-reactive autoantibodies may be involved in the pathogenesis of FPS.</p>","PeriodicalId":54630,"journal":{"name":"Pediatric Rheumatology","volume":"23 1","pages":"17"},"PeriodicalIF":2.3000,"publicationDate":"2025-02-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11834650/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Rheumatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12969-025-01071-w","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Fasciitis-panniculitis syndrome (FPS) typically presents with swelling and skin hardening. Its histopathological characteristics include inflammatory cell infiltration and fibrous thickening of the subcutaneous tissue and fascia. Panniculitides in children are rare and only a small number of juvenile FPS cases have been reported. We encountered a case of a 10-year-old boy in which autoantibodies reactive to adipocyte pericellular fibers were detected in relapsing FPS.
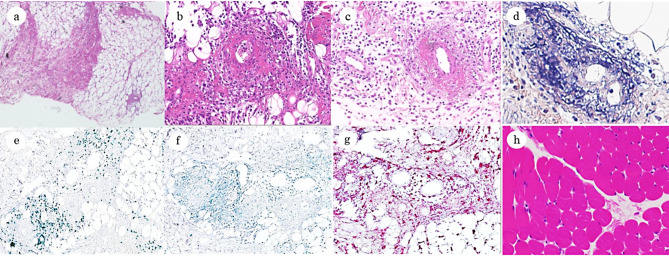
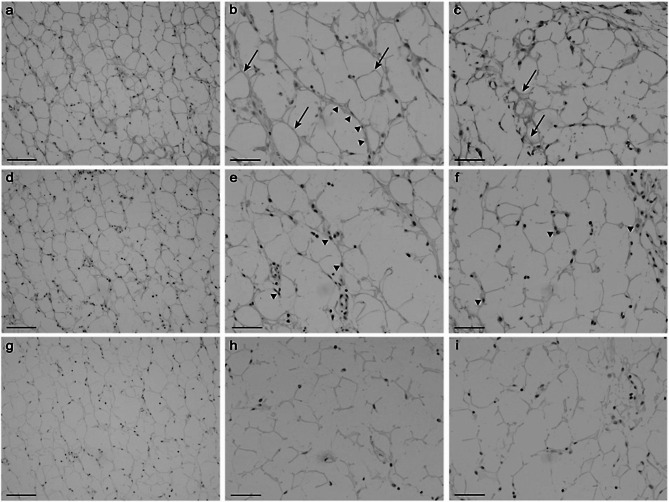
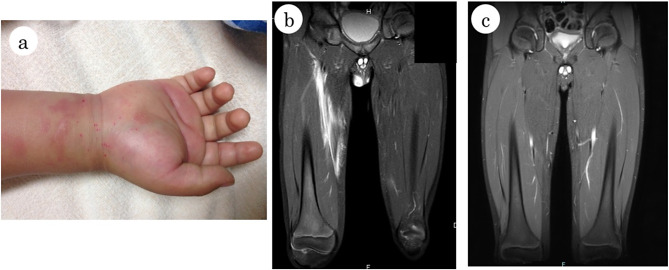
Case presentation: The patient developed a high fever and skin swelling with pain and erythema on the right side of his body following an abrasion injury on his right wrist at the age of 5 years, and was suspected of having streptococcal toxic shock-like syndrome, for which he received antimicrobials, immunoglobulin therapy, debridement, and plasma exchange. The same manifestations with similar magnetic resonance imaging (MRI) findings of high signal on short tau inversion recovery showing the spread of inflammation in the fat tissue and fascia was observed twice at the age of 6 years. Serological analyses for conventional autoantibodies, bone marrow aspiration, and whole-exome sequencing examination were non-remarkable. Prednisolone was effective in ameliorating the above putative autoinflammatory syndrome. The patient was admitted at the age of 10 years with similar clinical and MRI findings indicative of recurrence of the same disease. En bloc biopsy from the skin to the fascia showed thickening of collagen fibers, infiltration of inflammatory cells composed mainly of neutrophils and lymphocytes, and necrotizing vasculitis in the fat tissue and fascia. Immunohistochemical staining of the en bloc biopsy sections indicated infiltration of T lymphocytes and macrophages in the perivascular connective tissue and fibrinoid necrosis, supporting the diagnosis of FPS. Induction therapy with prednisolone resulted in a remission. IgG purified from the patient's serum reacted with pericellular basement membranes in the subcutaneous fat tissue by immunohistochemistry. The patient is currently taking famotidine to prevent relapses and is making good progress in his recovery.
Conclusions: Although pathogenic autoantibodies have not been described in FPS, our results suggest that fat-tissue-reactive autoantibodies may be involved in the pathogenesis of FPS.
期刊介绍:
Pediatric Rheumatology is an open access, peer-reviewed, online journal encompassing all aspects of clinical and basic research related to pediatric rheumatology and allied subjects.
The journal’s scope of diseases and syndromes include musculoskeletal pain syndromes, rheumatic fever and post-streptococcal syndromes, juvenile idiopathic arthritis, systemic lupus erythematosus, juvenile dermatomyositis, local and systemic scleroderma, Kawasaki disease, Henoch-Schonlein purpura and other vasculitides, sarcoidosis, inherited musculoskeletal syndromes, autoinflammatory syndromes, and others.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


