Kinal Paresh Bhatt, Larri Rudman, Daniela Ramos Padilla, Kamal Akbar, Nicole Clarke, Paulraj Rahulraj, George Michel
{"title":"A case report of long-term asymptomatic primary hypothyroidism treated with levothyroxine and dexamethasone.","authors":"Kinal Paresh Bhatt, Larri Rudman, Daniela Ramos Padilla, Kamal Akbar, Nicole Clarke, Paulraj Rahulraj, George Michel","doi":"10.15190/d.2024.5","DOIUrl":null,"url":null,"abstract":"<p><p>Hypothyroidism is an underactive thyroid gland that is diagnosed based on the laboratory findings. The risk is higher in women over the age of 60, pregnancy, patients with a prior history of head and neck irradiation, patients with autoimmune disorders and/or type 1 diabetes, family history, positive thyroid peroxidase antibodies, and medication adverse effects. The primary screening test for thyroid dysfunction is serum thyroid stimulating hormone (TSH) testing. Abnormal findings will require a follow-up testing of serum thyroxine (T4). Abnormally high TSH and low T4 will confirm the diagnosis of hypothyroidism, also known as \"overt\" hypothyroidism. No consensus exists on the treatment threshold or better clinical outcome for hypothyroidism. Generally, a TSH level greater than 10.0 mIU/L is considered optimal for treatment initiation for symptomatic and asymptomatic hypothyroid patients. The present case emphasizes the importance of close observation in a patient with primary hypothyroidism findings and the importance of adequate treatment. When treated with thyroxine replacement, both autoimmune and nonautoimmune mechanisms of primary hypothyroidism may contribute to iatrogenic thyrotoxicosis. Levothyroxine has a very narrow therapeutic index; therefore, to avoid adverse effects of levothyroxine-induced iatrogenic thyrotoxicosis, dexamethasone was added as an adjunct medication. Dexamethasone inhibits TSH, further reducing the release of T3 and T4 from the anterior pituitary gland. We advised the patient to have an outpatient follow-up for appropriate follow-up and educated him about the importance of continuity of care for his diagnosis.</p>","PeriodicalId":72829,"journal":{"name":"Discoveries (Craiova, Romania)","volume":"12 2","pages":"e186"},"PeriodicalIF":0.0000,"publicationDate":"2024-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11835451/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Discoveries (Craiova, Romania)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15190/d.2024.5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/4/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
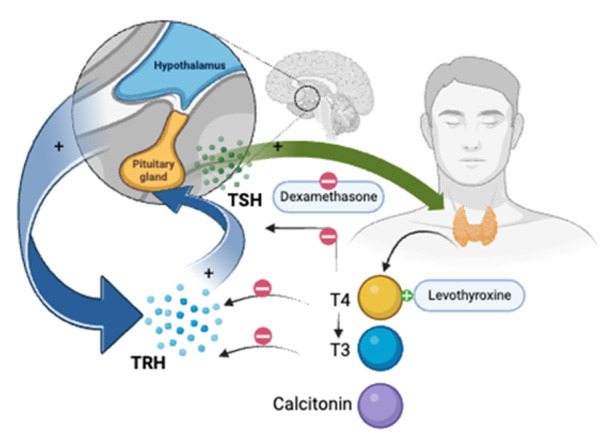
Hypothyroidism is an underactive thyroid gland that is diagnosed based on the laboratory findings. The risk is higher in women over the age of 60, pregnancy, patients with a prior history of head and neck irradiation, patients with autoimmune disorders and/or type 1 diabetes, family history, positive thyroid peroxidase antibodies, and medication adverse effects. The primary screening test for thyroid dysfunction is serum thyroid stimulating hormone (TSH) testing. Abnormal findings will require a follow-up testing of serum thyroxine (T4). Abnormally high TSH and low T4 will confirm the diagnosis of hypothyroidism, also known as "overt" hypothyroidism. No consensus exists on the treatment threshold or better clinical outcome for hypothyroidism. Generally, a TSH level greater than 10.0 mIU/L is considered optimal for treatment initiation for symptomatic and asymptomatic hypothyroid patients. The present case emphasizes the importance of close observation in a patient with primary hypothyroidism findings and the importance of adequate treatment. When treated with thyroxine replacement, both autoimmune and nonautoimmune mechanisms of primary hypothyroidism may contribute to iatrogenic thyrotoxicosis. Levothyroxine has a very narrow therapeutic index; therefore, to avoid adverse effects of levothyroxine-induced iatrogenic thyrotoxicosis, dexamethasone was added as an adjunct medication. Dexamethasone inhibits TSH, further reducing the release of T3 and T4 from the anterior pituitary gland. We advised the patient to have an outpatient follow-up for appropriate follow-up and educated him about the importance of continuity of care for his diagnosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


