Faizan Bashir, Moiza Bashir, Moniza Rafiq, Ali Jafer, Saide Honarmand
{"title":"Symmetrical polyarthritis in IgG4-related sialadenitis: a diagnostic challenge with seronegative rheumatoid arthritis.","authors":"Faizan Bashir, Moiza Bashir, Moniza Rafiq, Ali Jafer, Saide Honarmand","doi":"10.1186/s41927-025-00471-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>IgG4-related disease (IgG4-RD) is a systemic fibro-inflammatory condition characterized by elevated IgG4 serum levels and tissue infiltration by IgG4-positive plasma cells. While often presenting with organ-specific involvement, such as sialadenitis or pancreatitis, its rheumatologic manifestations are rare and poorly understood. IgG4-RD often overlaps with autoimmune diseases such as rheumatoid arthritis (RA), posing a diagnostic challenge, particularly in seronegative presentations.</p><p><strong>Case presentation: </strong>We report a 48-year-old male presenting with progressive symmetrical polyarthritis mimicking rheumatoid arthritis. Laboratory findings showed elevated serum IgG4 levels and inflammatory markers, while autoantibodies (RF, ACPA, ANA, ANCA) were negative. A biopsy of a submandibular gland revealed dense lymphoplasmacytic infiltrates + fibrosis and IgG4-positive plasma cells, confirming the diagnosis of IgG4-RD. The patient responded well to a combination of glucocorticoids and methotrexate, with complete symptom resolution within one month and normalization of inflammatory markers.The therapeutic response observed in this case demonstrates the effectiveness of immunosuppression therapy in IgG4-RD management, while emphasizing the need for long-term follow-up.</p><p><strong>Discussion: </strong>This case underscores the diagnostic challenges in recognizing arthritis in a patient with biopsy-confirmed IgG4-related sialadenitis particularly when seronegative rheumatoid arthritis (RA) remains a plausible differential diagnosis.The overlapping clinical features and shared treatment responses make it challenging to attribute the arthritis to a single etiology.This report emphasizes the importance of considering IgG4-RD in the differential diagnosis of atypical arthritis presentations, particularly in patients with systemic manifestations. Histopathological confirmation, supported by clinical and serological evaluation, remains pivotal in guiding diagnosis and management. Long-term follow-up is essential to monitor for evolving features, including the potential development of overlapping conditions, and to ensure optimal treatment outcomes. Early recognition and tailored interventions are critical to preventing complications and improving patient quality of life.</p><p><strong>Conclusion: </strong>IgG4-related disease (IgG4-RD) must be considered in the differential diagnosis of seronegative arthritis, especially when systemic symptoms or organ involvement are present. This case underscores the growing recognition of IgG4-RD in rheumatologic practice and the importance of a multidisciplinary approach to diagnosis and management. Clinicians should maintain heightened awareness of the overlap between IgG4-RD and rheumatoid arthritis (RA), advocating for the integration of histopathology, imaging, and serological testing to ensure accurate diagnosis. Additionally, long-term follow-up is essential to monitor disease progression, recurrence, development of new symptoms, and treatment response, ultimately enhancing patient care and outcomes.</p>","PeriodicalId":9150,"journal":{"name":"BMC Rheumatology","volume":"9 1","pages":"20"},"PeriodicalIF":2.5000,"publicationDate":"2025-02-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11834622/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41927-025-00471-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: IgG4-related disease (IgG4-RD) is a systemic fibro-inflammatory condition characterized by elevated IgG4 serum levels and tissue infiltration by IgG4-positive plasma cells. While often presenting with organ-specific involvement, such as sialadenitis or pancreatitis, its rheumatologic manifestations are rare and poorly understood. IgG4-RD often overlaps with autoimmune diseases such as rheumatoid arthritis (RA), posing a diagnostic challenge, particularly in seronegative presentations.
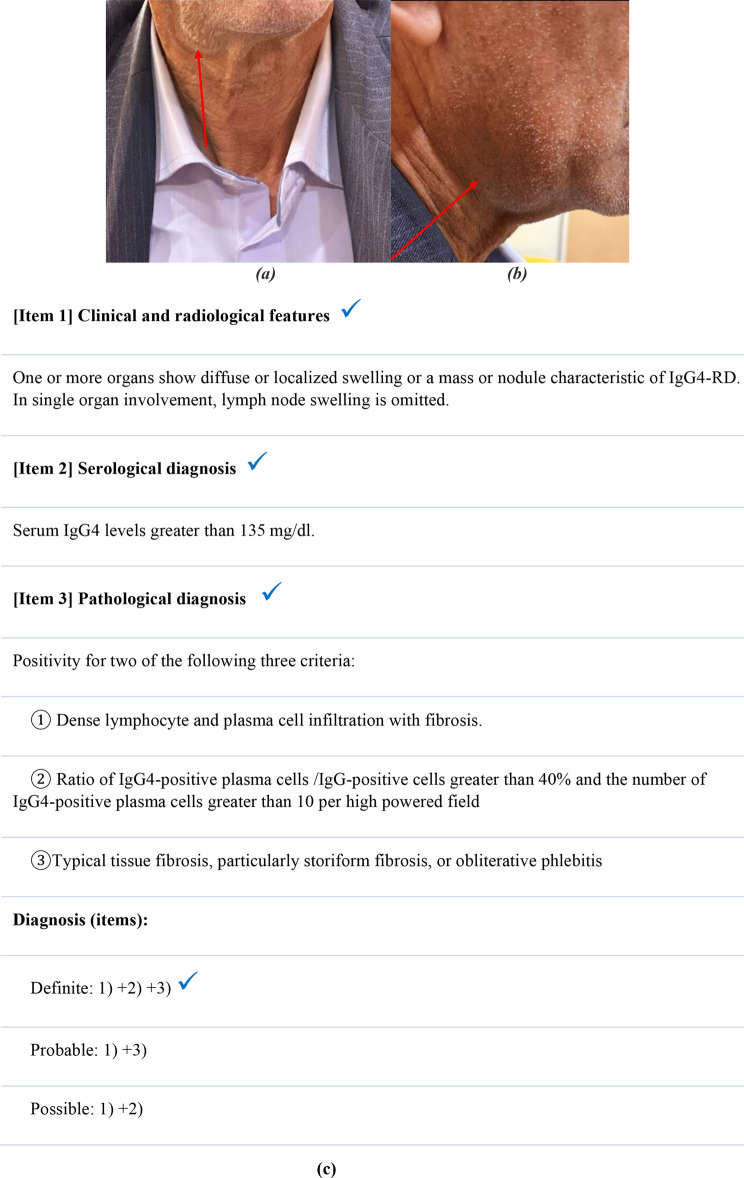
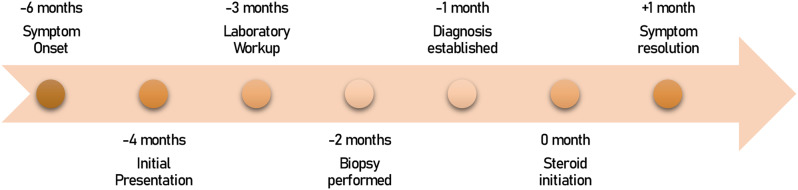
Case presentation: We report a 48-year-old male presenting with progressive symmetrical polyarthritis mimicking rheumatoid arthritis. Laboratory findings showed elevated serum IgG4 levels and inflammatory markers, while autoantibodies (RF, ACPA, ANA, ANCA) were negative. A biopsy of a submandibular gland revealed dense lymphoplasmacytic infiltrates + fibrosis and IgG4-positive plasma cells, confirming the diagnosis of IgG4-RD. The patient responded well to a combination of glucocorticoids and methotrexate, with complete symptom resolution within one month and normalization of inflammatory markers.The therapeutic response observed in this case demonstrates the effectiveness of immunosuppression therapy in IgG4-RD management, while emphasizing the need for long-term follow-up.
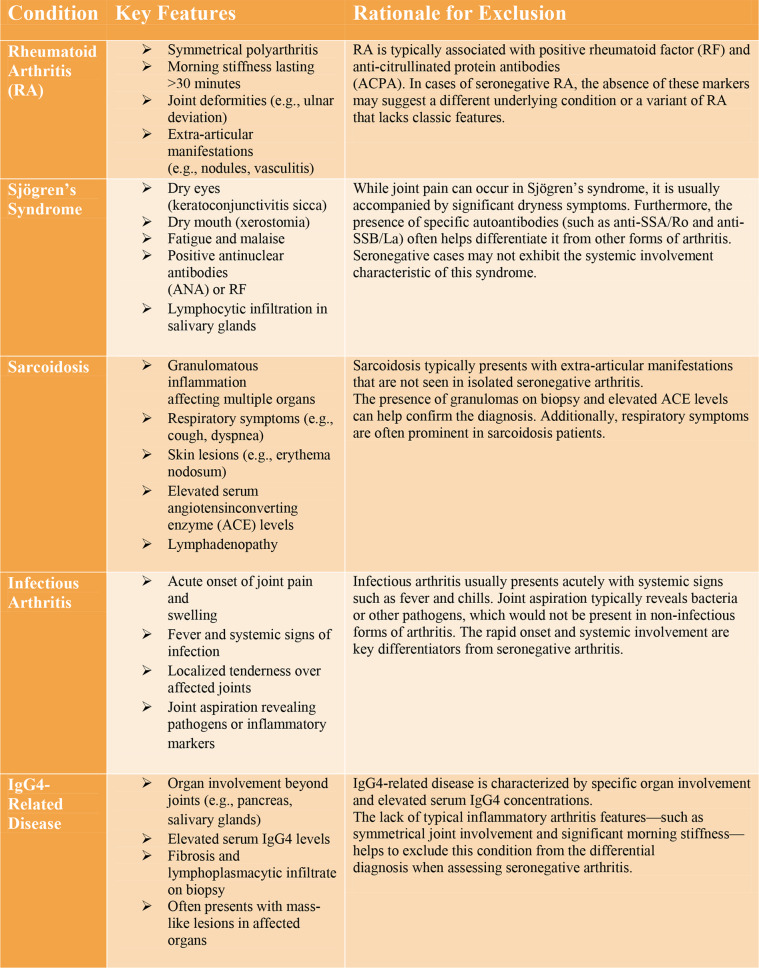
Discussion: This case underscores the diagnostic challenges in recognizing arthritis in a patient with biopsy-confirmed IgG4-related sialadenitis particularly when seronegative rheumatoid arthritis (RA) remains a plausible differential diagnosis.The overlapping clinical features and shared treatment responses make it challenging to attribute the arthritis to a single etiology.This report emphasizes the importance of considering IgG4-RD in the differential diagnosis of atypical arthritis presentations, particularly in patients with systemic manifestations. Histopathological confirmation, supported by clinical and serological evaluation, remains pivotal in guiding diagnosis and management. Long-term follow-up is essential to monitor for evolving features, including the potential development of overlapping conditions, and to ensure optimal treatment outcomes. Early recognition and tailored interventions are critical to preventing complications and improving patient quality of life.
Conclusion: IgG4-related disease (IgG4-RD) must be considered in the differential diagnosis of seronegative arthritis, especially when systemic symptoms or organ involvement are present. This case underscores the growing recognition of IgG4-RD in rheumatologic practice and the importance of a multidisciplinary approach to diagnosis and management. Clinicians should maintain heightened awareness of the overlap between IgG4-RD and rheumatoid arthritis (RA), advocating for the integration of histopathology, imaging, and serological testing to ensure accurate diagnosis. Additionally, long-term follow-up is essential to monitor disease progression, recurrence, development of new symptoms, and treatment response, ultimately enhancing patient care and outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


