Double Band Ligation-Assisted Endoscopic Submucosal Resection for Rectal Neuroendocrine Tumors: Comparison With Conventional Endoscopic Mucosal Resection With Ligation (With Video).
Yuan Gao, Liansong Ye, Xu Li, Long He, Bin Yu, Wei Liu, Yuwan Cao, Liuxiang Chen, Yi Mou, Ou Chen, Jia Xie, Jiang Du, Qiongying Zhang, Bing Hu
{"title":"Double Band Ligation-Assisted Endoscopic Submucosal Resection for Rectal Neuroendocrine Tumors: Comparison With Conventional Endoscopic Mucosal Resection With Ligation (With Video).","authors":"Yuan Gao, Liansong Ye, Xu Li, Long He, Bin Yu, Wei Liu, Yuwan Cao, Liuxiang Chen, Yi Mou, Ou Chen, Jia Xie, Jiang Du, Qiongying Zhang, Bing Hu","doi":"10.14309/ctg.0000000000000830","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Based on endoscopic mucosal resection with ligation (EMR-L), we developed double band ligation-assisted endoscopic submucosal resection (ESR) for complete resection of small submucosal rectal neuroendocrine tumors (NETs). Both procedures use a multiband device to perform resection, with the only difference being that ESR adds an additional band to obtain deeper resection margin. The aim of this retrospective study was to validate its feasibility, safety, and effectiveness compared with EMR-L.</p><p><strong>Methods: </strong>This retrospective study included consecutive patients with small (≤10 mm) suspected submucosal rectal NETs who underwent ESR (n = 45) or EMR-L (n = 26) between June 2018 and October 2023 at West China Hospital. En bloc resection rate, complete resection rate, procedure time, margin distance, and adverse events were compared between 2 groups.</p><p><strong>Results: </strong>En bloc resections were achieved in all patients. The complete resection rate of ESR was higher than EMR-L (100% vs 88.5%, P = 0.045). The vertical margin distance and lateral margin distance were significantly longer in ESR group than EMR-L group (vertical margin distance 782.31 ± 359.45 μm vs 363.84 ± 222.78 μm, P < 0.001; and lateral margin distance 4,205.75 ± 2,167.43 μm vs 3,162.94 ± 1,419.22 μm, P = 0.008, respectively). There were no significant differences in procedure time, adverse events, postprocedural hospital stay, or medical cost between 2 groups. In addition, there was no evidence of recurrence or metastasis during the follow-up.</p><p><strong>Discussion: </strong>ESR seems to be safe and effective for complete resection of small submucosal rectal NETs. Larger, multicenter, prospective studies are needed to further assess this technique.</p>","PeriodicalId":10278,"journal":{"name":"Clinical and Translational Gastroenterology","volume":" ","pages":"e00830"},"PeriodicalIF":3.0000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12101914/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Translational Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14309/ctg.0000000000000830","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
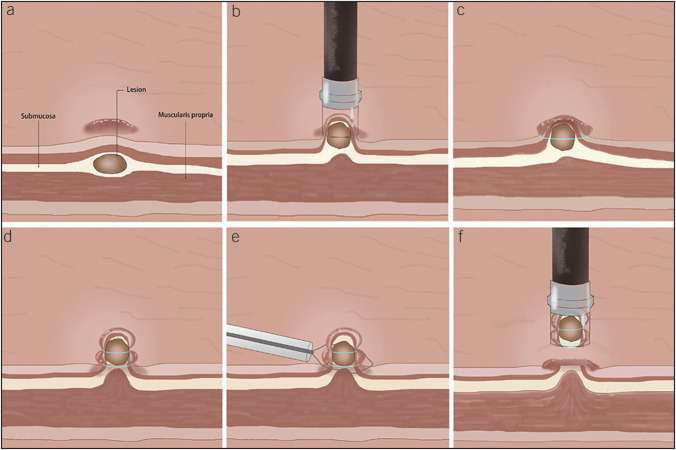
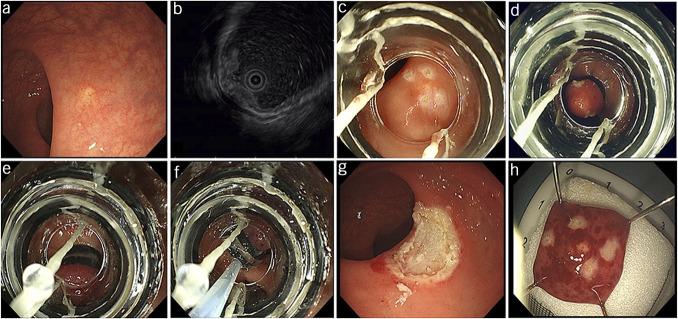
Introduction: Based on endoscopic mucosal resection with ligation (EMR-L), we developed double band ligation-assisted endoscopic submucosal resection (ESR) for complete resection of small submucosal rectal neuroendocrine tumors (NETs). Both procedures use a multiband device to perform resection, with the only difference being that ESR adds an additional band to obtain deeper resection margin. The aim of this retrospective study was to validate its feasibility, safety, and effectiveness compared with EMR-L.
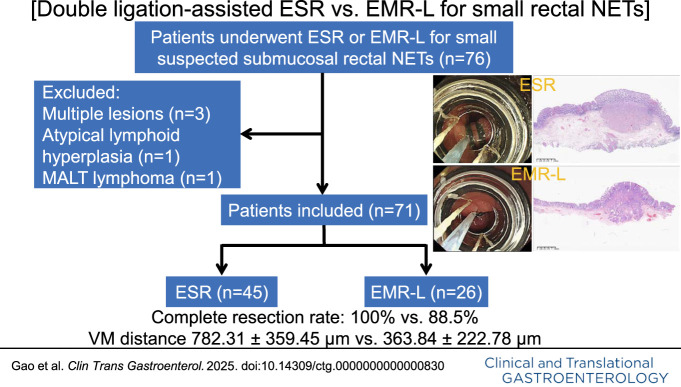
Methods: This retrospective study included consecutive patients with small (≤10 mm) suspected submucosal rectal NETs who underwent ESR (n = 45) or EMR-L (n = 26) between June 2018 and October 2023 at West China Hospital. En bloc resection rate, complete resection rate, procedure time, margin distance, and adverse events were compared between 2 groups.
Results: En bloc resections were achieved in all patients. The complete resection rate of ESR was higher than EMR-L (100% vs 88.5%, P = 0.045). The vertical margin distance and lateral margin distance were significantly longer in ESR group than EMR-L group (vertical margin distance 782.31 ± 359.45 μm vs 363.84 ± 222.78 μm, P < 0.001; and lateral margin distance 4,205.75 ± 2,167.43 μm vs 3,162.94 ± 1,419.22 μm, P = 0.008, respectively). There were no significant differences in procedure time, adverse events, postprocedural hospital stay, or medical cost between 2 groups. In addition, there was no evidence of recurrence or metastasis during the follow-up.
Discussion: ESR seems to be safe and effective for complete resection of small submucosal rectal NETs. Larger, multicenter, prospective studies are needed to further assess this technique.
背景与目的:在内镜粘膜结扎切除术(EMR-L)的基础上,我们发展了双带结扎辅助内镜粘膜下切除术(ESR),用于直肠粘膜下小神经内分泌肿瘤(NETs)的全切除术。两种手术都使用多波段设备进行切除,唯一的区别是ESR增加了额外的波段以获得更深的切除余量。本回顾性研究旨在验证其与EMR-L比较的可行性、安全性和有效性。方法:本回顾性研究包括2018年6月至2023年10月在华西医院连续接受ESR (n=45)或EMR-L (n=26)的疑似小(≤10 mm)粘膜下直肠NETs患者。比较两组的整体切除率、完全切除率、手术时间、切缘距离和不良事件。结果:所有患者均实现了整体切除。ESR的全切率高于EMR-L (100% vs. 88.5%, P=0.045)。ESR组垂直切缘(VM)距离和侧切缘(LM)距离明显长于EMR-L组(VM距离782.31±359.45 μm vs. 363.84±222.78 μm, P < 0.001;LM距离分别为4205.75±2167.43 μm和3162.94±1419.22 μm, P = 0.008)。两组在手术时间、不良事件、术后住院时间或医疗费用方面无显著差异。此外,随访期间无复发或转移的证据。结论:ESR对于直肠粘膜下小网的完全切除是安全有效的。需要更大的、多中心的前瞻性研究来进一步评估这种技术。
期刊介绍:
Clinical and Translational Gastroenterology (CTG), published on behalf of the American College of Gastroenterology (ACG), is a peer-reviewed open access online journal dedicated to innovative clinical work in the field of gastroenterology and hepatology. CTG hopes to fulfill an unmet need for clinicians and scientists by welcoming novel cohort studies, early-phase clinical trials, qualitative and quantitative epidemiologic research, hypothesis-generating research, studies of novel mechanisms and methodologies including public health interventions, and integration of approaches across organs and disciplines. CTG also welcomes hypothesis-generating small studies, methods papers, and translational research with clear applications to human physiology or disease.
Colon and small bowel
Endoscopy and novel diagnostics
Esophagus
Functional GI disorders
Immunology of the GI tract
Microbiology of the GI tract
Inflammatory bowel disease
Pancreas and biliary tract
Liver
Pathology
Pediatrics
Preventative medicine
Nutrition/obesity
Stomach.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


