{"title":"Parenchymal-sparing non-anatomic resection vs. classic anatomic resection in colorectal cancer liver metastases.","authors":"Sungwon Jung","doi":"10.14701/ahbps.24-151","DOIUrl":null,"url":null,"abstract":"<p><strong>Backgrounds/aims: </strong>Although anatomical liver resection is considered more effective in preventing complications and recurrence in hepatocellular carcinoma, its efficacy has yet to be clearly defined in colorectal cancer liver metastasis (CLM).</p><p><strong>Methods: </strong>From January 2000 to December 2023, 145 patients underwent liver resections for CLM, divided into anatomic and non-anatomic resection cohorts. The dataset included demographic details, tumor size, number and distribution of metastases, neoadjuvant chemotherapy, primary tumor location and stage, type of liver surgery, transfusion rates, duration of hospital stay, postoperative complications, and completeness of resection.</p><p><strong>Results: </strong>Of the 145 patients who underwent liver resections for metastases from colorectal cancer, 62 were in the anatomic group and 83 were in the non-anatomic group. The anatomic group had larger tumors (6.71 cm vs. 3.18 cm). Intraoperative transfusion rates were higher in the anatomic group (56.5% vs. 12.0%). Hospital stays, positive resection margin rates, and postoperative complication rates showed no significant differences. One surgery-related death occurred in the anatomic group. Disease-free and overall survival rates were comparable between groups.</p><p><strong>Conclusions: </strong>Anatomic liver resection did not demonstrate a reduction in recurrence or an improvement in survival rates compared to non-anatomic resection. As such, anatomical resection does not offer a <i>survival</i> advantage over non-anatomical resection. Consequently, surgical method selection should prioritize patient safety, preservation of residual liver parenchyma, and tumor-specific factors.</p>","PeriodicalId":72220,"journal":{"name":"Annals of hepato-biliary-pancreatic surgery","volume":" ","pages":"121-126"},"PeriodicalIF":1.7000,"publicationDate":"2025-05-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12093235/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of hepato-biliary-pancreatic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14701/ahbps.24-151","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/18 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Backgrounds/aims: Although anatomical liver resection is considered more effective in preventing complications and recurrence in hepatocellular carcinoma, its efficacy has yet to be clearly defined in colorectal cancer liver metastasis (CLM).
Methods: From January 2000 to December 2023, 145 patients underwent liver resections for CLM, divided into anatomic and non-anatomic resection cohorts. The dataset included demographic details, tumor size, number and distribution of metastases, neoadjuvant chemotherapy, primary tumor location and stage, type of liver surgery, transfusion rates, duration of hospital stay, postoperative complications, and completeness of resection.
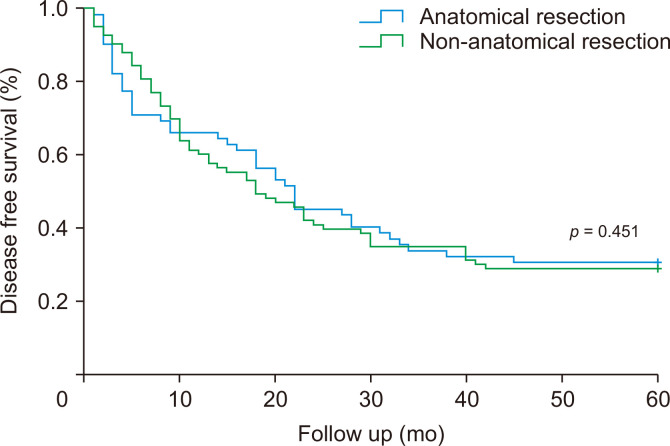
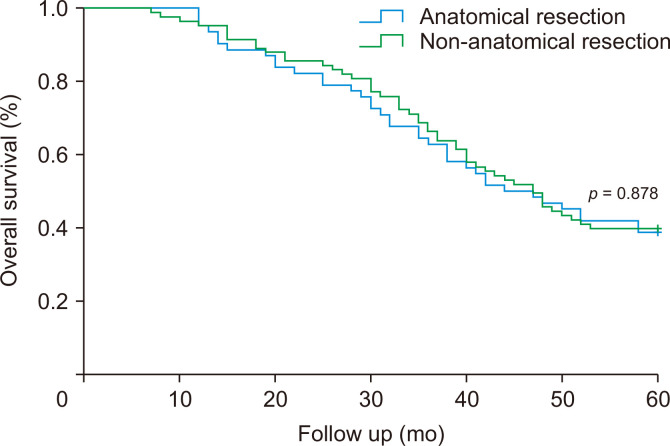
Results: Of the 145 patients who underwent liver resections for metastases from colorectal cancer, 62 were in the anatomic group and 83 were in the non-anatomic group. The anatomic group had larger tumors (6.71 cm vs. 3.18 cm). Intraoperative transfusion rates were higher in the anatomic group (56.5% vs. 12.0%). Hospital stays, positive resection margin rates, and postoperative complication rates showed no significant differences. One surgery-related death occurred in the anatomic group. Disease-free and overall survival rates were comparable between groups.
Conclusions: Anatomic liver resection did not demonstrate a reduction in recurrence or an improvement in survival rates compared to non-anatomic resection. As such, anatomical resection does not offer a survival advantage over non-anatomical resection. Consequently, surgical method selection should prioritize patient safety, preservation of residual liver parenchyma, and tumor-specific factors.
背景/目的:虽然解剖性肝切除术被认为在预防肝细胞癌并发症和复发方面更有效,但其在结直肠癌肝转移(CLM)中的疗效尚未明确。方法:2000年1月至2023年12月,145例CLM患者行肝切除术,分为解剖和非解剖两组。数据集包括人口统计学细节、肿瘤大小、转移的数量和分布、新辅助化疗、原发肿瘤的位置和分期、肝脏手术类型、输血率、住院时间、术后并发症和切除的完整性。结果:145例结直肠癌转移肝切除术患者中,解剖组62例,非解剖组83例。解剖组肿瘤较大(6.71 cm vs. 3.18 cm)。解剖组术中输血率较高(56.5%比12.0%)。住院时间、阳性切缘率和术后并发症发生率无显著差异。解剖组发生一例手术相关死亡。两组间无病生存率和总生存率具有可比性。结论:与非解剖性肝切除术相比,解剖性肝切除术并没有减少复发或提高生存率。因此,解剖切除并不比非解剖切除提供生存优势。因此,手术方法的选择应优先考虑患者安全、保留残余肝实质和肿瘤特异性因素。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


