Markus Lauerer, Tun Wiltgen, Carolin Brückner, Christina Engl, Katrin Giglhuber, Sebastian Lambrecht, Viola Pongratz, Achim Berthele, Christiane Gasperi, Jan S Kirschke, Claus Zimmer, Bernhard Hemmer, Mark Mühlau
{"title":"Predictors of early disability accumulation in newly diagnosed multiple sclerosis: clinical, imaging and cerebrospinal fluid measures.","authors":"Markus Lauerer, Tun Wiltgen, Carolin Brückner, Christina Engl, Katrin Giglhuber, Sebastian Lambrecht, Viola Pongratz, Achim Berthele, Christiane Gasperi, Jan S Kirschke, Claus Zimmer, Bernhard Hemmer, Mark Mühlau","doi":"10.1136/jnnp-2024-335037","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A growing arsenal of treatment options for relapsing multiple sclerosis (RMS) emphasises the need for early prognostic biomarkers. While evidence for individual markers exists, comprehensive analyses at the time of diagnosis are sparse.</p><p><strong>Methods: </strong>Brain and spinal cord lesion numbers, cerebrospinal fluid parameters, initial symptoms, and Expanded Disability Status Scale (EDSS) score were determined at the time of diagnosis. Confirmed disability accumulation (CDA), defined as a sustained EDSS increase over 6 months, was determined during a 5-year follow-up. All-subsets multivariable logistic regression was performed to identify predictors of CDA. Model performance was assessed via receiver operating characteristic analysis, and individual risks were calculated. Analyses were repeated with progression independent of relapse activity (PIRA) as an outcome.</p><p><strong>Results: </strong>113/417 (27.1%) people with RMS experienced CDA on follow-up. Intrathecal IgG synthesis, a higher number of spinal cord lesions, age and polysymptomatic manifestation were identified as independent predictors of CDA. The resulting prediction model yielded an area under the curve (AUC) of 0.75 with a 95% CI of 0.70 to 0.80. Individuals exceeding the optimal thresholds for the three most significant predictors had a 61.8% likelihood of experiencing CDA, whereas those below all three thresholds had a CDA rate of 4.5%. The only significant baseline predictor differentiating PIRA from relapse-associated worsening was a higher number of spinal cord lesions (AUC=0.64, 95% CI 0.54 to 0.74).</p><p><strong>Conclusions: </strong>Intrathecal IgG synthesis, spinal cord lesion number, age and polysymptomatic manifestation are independent predictors of early CDA in newly diagnosed RMS.</p>","PeriodicalId":16418,"journal":{"name":"Journal of Neurology, Neurosurgery, and Psychiatry","volume":" ","pages":"900-907"},"PeriodicalIF":7.5000,"publicationDate":"2025-08-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12418557/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurology, Neurosurgery, and Psychiatry","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/jnnp-2024-335037","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: A growing arsenal of treatment options for relapsing multiple sclerosis (RMS) emphasises the need for early prognostic biomarkers. While evidence for individual markers exists, comprehensive analyses at the time of diagnosis are sparse.
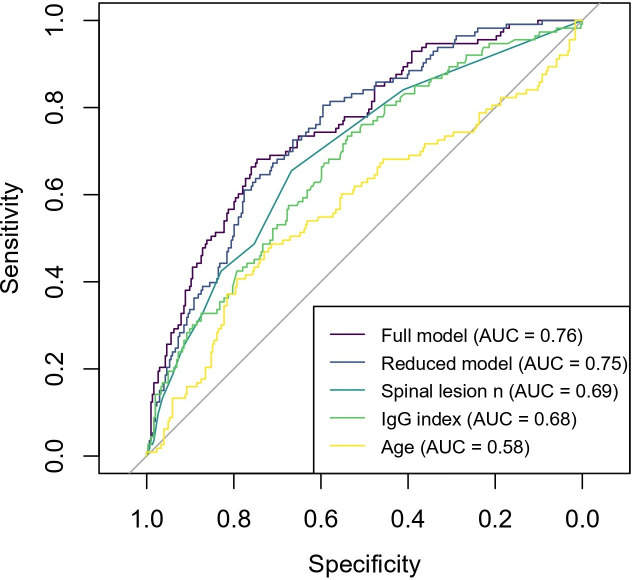
Methods: Brain and spinal cord lesion numbers, cerebrospinal fluid parameters, initial symptoms, and Expanded Disability Status Scale (EDSS) score were determined at the time of diagnosis. Confirmed disability accumulation (CDA), defined as a sustained EDSS increase over 6 months, was determined during a 5-year follow-up. All-subsets multivariable logistic regression was performed to identify predictors of CDA. Model performance was assessed via receiver operating characteristic analysis, and individual risks were calculated. Analyses were repeated with progression independent of relapse activity (PIRA) as an outcome.
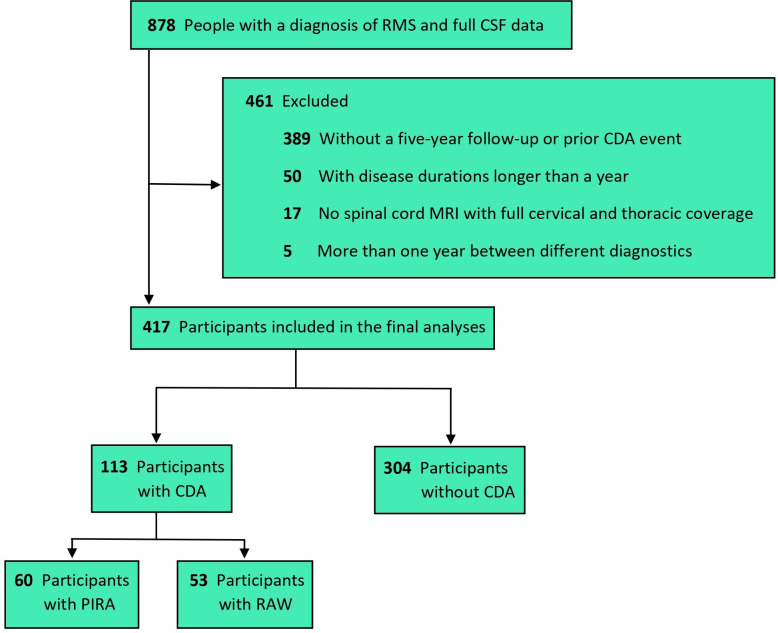
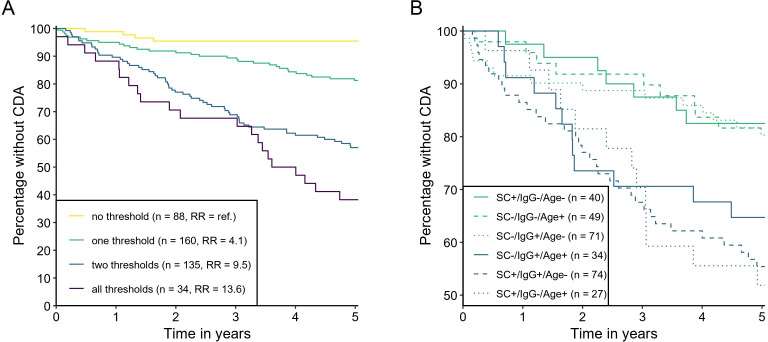
Results: 113/417 (27.1%) people with RMS experienced CDA on follow-up. Intrathecal IgG synthesis, a higher number of spinal cord lesions, age and polysymptomatic manifestation were identified as independent predictors of CDA. The resulting prediction model yielded an area under the curve (AUC) of 0.75 with a 95% CI of 0.70 to 0.80. Individuals exceeding the optimal thresholds for the three most significant predictors had a 61.8% likelihood of experiencing CDA, whereas those below all three thresholds had a CDA rate of 4.5%. The only significant baseline predictor differentiating PIRA from relapse-associated worsening was a higher number of spinal cord lesions (AUC=0.64, 95% CI 0.54 to 0.74).
Conclusions: Intrathecal IgG synthesis, spinal cord lesion number, age and polysymptomatic manifestation are independent predictors of early CDA in newly diagnosed RMS.
背景:复发性多发性硬化症(RMS)的治疗选择越来越多,这强调了对早期预后生物标志物的需求。虽然存在个体标记物的证据,但诊断时的综合分析很少。方法:在诊断时测定脑和脊髓病变数、脑脊液参数、初始症状和扩展残疾状态量表(EDSS)评分。确认的残疾积累(CDA),定义为EDSS持续增加超过6个月,在5年随访期间确定。采用全子集多变量logistic回归来确定CDA的预测因子。通过受试者操作特征分析评估模型性能,并计算个体风险。以独立于复发活动的进展(PIRA)作为结果重复分析。结果:417例RMS患者中有113例(27.1%)出现CDA。鞘内IgG合成、较高数量的脊髓病变、年龄和多症状表现被认为是CDA的独立预测因素。所得预测模型的曲线下面积(AUC)为0.75,95% CI为0.70至0.80。超过三个最重要预测指标的最佳阈值的个体经历CDA的可能性为61.8%,而低于三个阈值的个体的CDA率为4.5%。区分PIRA与复发相关恶化的唯一重要基线预测指标是脊髓病变数量较多(AUC=0.64, 95% CI 0.54至0.74)。结论:鞘内IgG合成、脊髓病变数量、年龄和多症状表现是新诊断RMS早期CDA的独立预测因素。
期刊介绍:
The Journal of Neurology, Neurosurgery & Psychiatry (JNNP) aspires to publish groundbreaking and cutting-edge research worldwide. Covering the entire spectrum of neurological sciences, the journal focuses on common disorders like stroke, multiple sclerosis, Parkinson’s disease, epilepsy, peripheral neuropathy, subarachnoid haemorrhage, and neuropsychiatry, while also addressing complex challenges such as ALS. With early online publication, regular podcasts, and an extensive archive collection boasting the longest half-life in clinical neuroscience journals, JNNP aims to be a trailblazer in the field.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


