{"title":"Spigelian Hernia in Cirrhotic Patients: When and How to Repair?","authors":"Nosibah Telmesani, Dhuha Boumarah, Naif Alkhaldi, Humood Alsadery, Saleh Busbait, Anas AlOthman, Faten Alaqeel","doi":"10.5455/aim.2024.32.126-129","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Spigelian hernia, also known as spontaneous lateral ventral hernia, is defined as a protrusion of abdominal contents through an abdominal wall defect within the transversus aponeurosis. The entity was first reported in 1742 and named after Adrian van der Spieghel. It is recognized as a rare condition, accounting for 1 to 2% of all abdominal wall hernias. Cirrhotic patients, in particular, are more predisposed to hernias of all types. When Spigelian hernia is accompanied by hepatic cirrhosis, the decision to repair gets into a controversial aspect. Herein, we present the emergency management of an incarcerated spigelian hernia in a cirrhotic patient, highlighting the challenges in managing similar cases.</p><p><strong>Case presentation: </strong>A 65-year-old lady, presented to our emergency department complaining of a left lower quadrant (LLQ) abdominal pain associated with a painful swelling for 9 hours duration. Upon assessment, the patient was jaundiced and haemodynamically stable. Abdominal examination revealed a soft and lax but distended abdomen, with irreducible tender swelling over the LLQ, measuring around 3x2 cm. Laboratory investigations showed anemia, hypoalbuminemia, hyperbilirubinemia, lactic acidosis and prolonged coagulation profile. A contrast-enhanced computed tomography (CT) scan of the abdomen showed evidence of incarcerated left spigelian hernia. Moreover, advanced cirrhosis of the liver was detected with hypertrophy of the caudate lobe, extensive ascites and splenomegaly. After establishing the diagnosis of incarcerated spigelian hernia, with a picture of advanced liver cirrhosis, Child-Pugh-Turcotte (CPT) score of C and a Model for End-Stage Liver Disease (MELD) score of 19 and Mayo score for post-operative mortality of 16% in 7 days and 53% in 30 days. Given the patient's condition which necessitates urgent operative intervention beside the risk of decompensation of pre-existing liver disease and high mortality. Decision was made to proceed with laparoscopic hernia repair. Intraoperatively, ischemic small bowel segment was resected with creation of end ileostomy. Conventional anatomical repair of the hernia defect was performed. Postoperatively, the patient was managed and resuscitated in critical care unit and then discharged home in a satisfactory condition on post-operative day 15. She passed away prior to liver transplantation, thirty-two days post-operatively in a different institution.</p><p><strong>Conclusion: </strong>The surgical management of complicated hernias in an emergency setting comprise a notable number of cases encountered by surgeons. It always needs special attention. Moreover, cirrhotic patients with their predicted high morbidity and mortality require even further vigilance. Therefore, a patient-tailored approach is always recommended when managing similar cases to provide optimal outcomes.</p>","PeriodicalId":7074,"journal":{"name":"Acta Informatica Medica","volume":"32 2","pages":"126-129"},"PeriodicalIF":0.0000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11821568/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta Informatica Medica","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5455/aim.2024.32.126-129","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Spigelian hernia, also known as spontaneous lateral ventral hernia, is defined as a protrusion of abdominal contents through an abdominal wall defect within the transversus aponeurosis. The entity was first reported in 1742 and named after Adrian van der Spieghel. It is recognized as a rare condition, accounting for 1 to 2% of all abdominal wall hernias. Cirrhotic patients, in particular, are more predisposed to hernias of all types. When Spigelian hernia is accompanied by hepatic cirrhosis, the decision to repair gets into a controversial aspect. Herein, we present the emergency management of an incarcerated spigelian hernia in a cirrhotic patient, highlighting the challenges in managing similar cases.
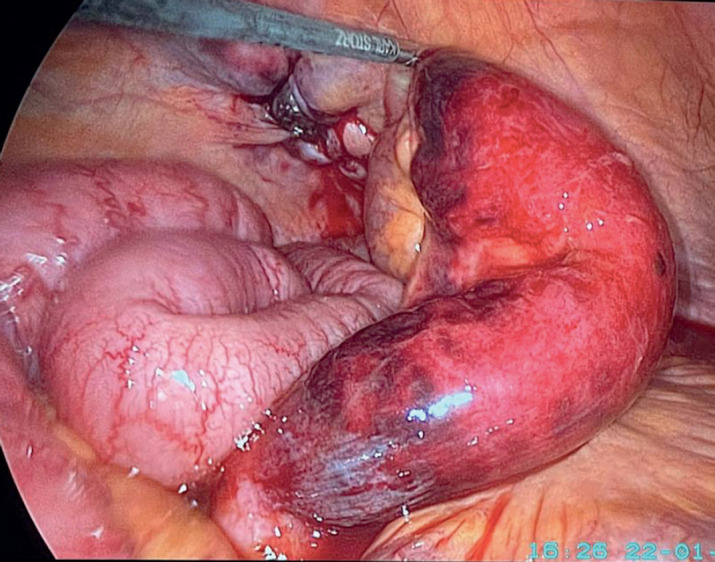
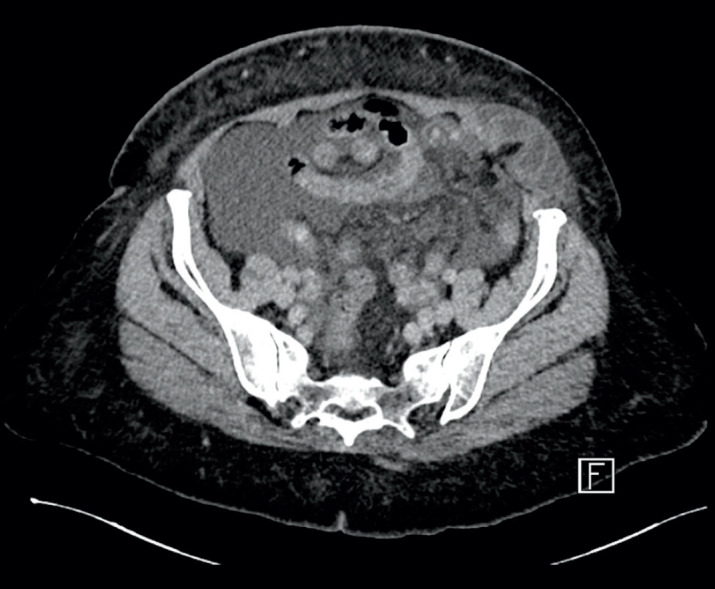
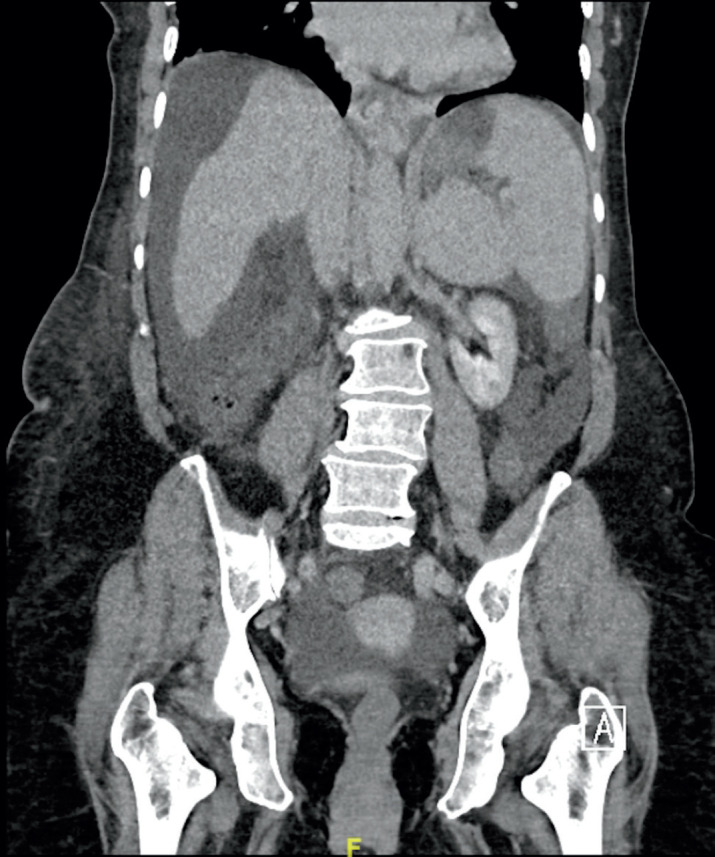
Case presentation: A 65-year-old lady, presented to our emergency department complaining of a left lower quadrant (LLQ) abdominal pain associated with a painful swelling for 9 hours duration. Upon assessment, the patient was jaundiced and haemodynamically stable. Abdominal examination revealed a soft and lax but distended abdomen, with irreducible tender swelling over the LLQ, measuring around 3x2 cm. Laboratory investigations showed anemia, hypoalbuminemia, hyperbilirubinemia, lactic acidosis and prolonged coagulation profile. A contrast-enhanced computed tomography (CT) scan of the abdomen showed evidence of incarcerated left spigelian hernia. Moreover, advanced cirrhosis of the liver was detected with hypertrophy of the caudate lobe, extensive ascites and splenomegaly. After establishing the diagnosis of incarcerated spigelian hernia, with a picture of advanced liver cirrhosis, Child-Pugh-Turcotte (CPT) score of C and a Model for End-Stage Liver Disease (MELD) score of 19 and Mayo score for post-operative mortality of 16% in 7 days and 53% in 30 days. Given the patient's condition which necessitates urgent operative intervention beside the risk of decompensation of pre-existing liver disease and high mortality. Decision was made to proceed with laparoscopic hernia repair. Intraoperatively, ischemic small bowel segment was resected with creation of end ileostomy. Conventional anatomical repair of the hernia defect was performed. Postoperatively, the patient was managed and resuscitated in critical care unit and then discharged home in a satisfactory condition on post-operative day 15. She passed away prior to liver transplantation, thirty-two days post-operatively in a different institution.
Conclusion: The surgical management of complicated hernias in an emergency setting comprise a notable number of cases encountered by surgeons. It always needs special attention. Moreover, cirrhotic patients with their predicted high morbidity and mortality require even further vigilance. Therefore, a patient-tailored approach is always recommended when managing similar cases to provide optimal outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


