Lucia D Beissel, Fabian Kording, Christian Ruprecht, Alexander Isaak, Thomas M Vollbrecht, Claus C Pieper, Daniel Kuetting, Abdulamir Ali, Pia Wölfl, Christopher Hart, Julian A Luetkens
{"title":"Doppler ultrasound gating for adult cardiovascular magnetic resonance: Initial experience.","authors":"Lucia D Beissel, Fabian Kording, Christian Ruprecht, Alexander Isaak, Thomas M Vollbrecht, Claus C Pieper, Daniel Kuetting, Abdulamir Ali, Pia Wölfl, Christopher Hart, Julian A Luetkens","doi":"10.1016/j.jocmr.2025.101862","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Despite being a common gating method for cardiovascular magnetic resonance (CMR), electrocardiogram (ECG) gating has its disadvantages, and new gating strategies are desirable. An alternative CMR gating method is Doppler ultrasound (DUS) gating, which detects blood flow and ventricular movement. The aim of this study was to prove the feasibility of DUS gating as a novel CMR gating method in a clinical patient population.</p><p><strong>Methods: </strong>In this prospective study, patients underwent clinically indicated CMR. Balanced steady-state free precession two-dimensional cine sequences in short-axis and 4-chamber views were acquired using ECG and DUS gating. DUS and ECG signal were recorded simultaneously. Time difference between R-wave and DUS systolic trigger detection was defined as trigger delay, the standard deviation of trigger delays as trigger jitter. Left and right ventricular parameters were assessed: left and right ventricular ejection fraction (LVEF, RVEF) and left and right ventricular end-diastolic volume index (LVEDVI, RVEDVI). Overall image quality was assessed using a 5-point Likert scale (5 = excellent to 1 = non-diagnostic). For statistical analysis, paired t-test, Wilcoxon test, Pearson correlation, and intraclass correlation coefficient (ICC) were employed.</p><p><strong>Results: </strong>Twenty-one patients (7 female) were included (age: 45.4 ± 19.7 years; body mass index: 27.6 ± 5.5 kg/m<sup>2</sup>). DUS mean trigger delay was 128 ± 28 ms. DUS mean trigger jitter was 23 ± 13 ms. Overall image quality showed no difference between ECG and DUS gating (e.g., short axis: 5 [interquartile range (IQR) 3-5] vs 4 [IQR 3.5-5]; P = 0.21). Quantitative analysis revealed no differences between ECG and DUS gating: LVEF (53.2 ± 9.2% vs 52.3 ± 9.1%; P = 0.18; ICC 0.97 [95% confidence interval [CI] 0.93-0.99]), LVEDVI (84.5 ± 15.8 mL/m<sup>2</sup> vs 83.3 ± 15.8 mL/m<sup>2</sup>; P = 0.06; ICC 0.99 [95% CI 0.98-1.00]), RVEF (52.8 ± 8.0% vs 51.6 ± 7.2%; P = 0.06; ICC 0.96 [95% CI 0.89-0.99]), and RVEDVI (80.8 ± 17.6 mL/m<sup>2</sup> vs 80.9 ± 16.5 mL/m<sup>2</sup>; P = 0.91; ICC 0.98 [95% CI 0.96-0.99]). In one patient with a prominent lingula of the lung image quality was non-diagnostic with DUS gating.</p><p><strong>Conclusion: </strong>CMR gating with DUS is feasible and can offer an equivalent performance to ECG regarding image quality and quantitative parameter assessment.</p>","PeriodicalId":15221,"journal":{"name":"Journal of Cardiovascular Magnetic Resonance","volume":" ","pages":"101862"},"PeriodicalIF":6.1000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12019829/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Magnetic Resonance","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.jocmr.2025.101862","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/13 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
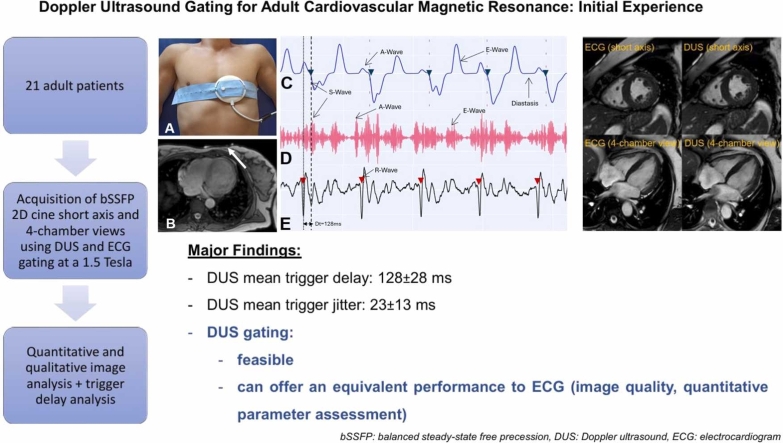
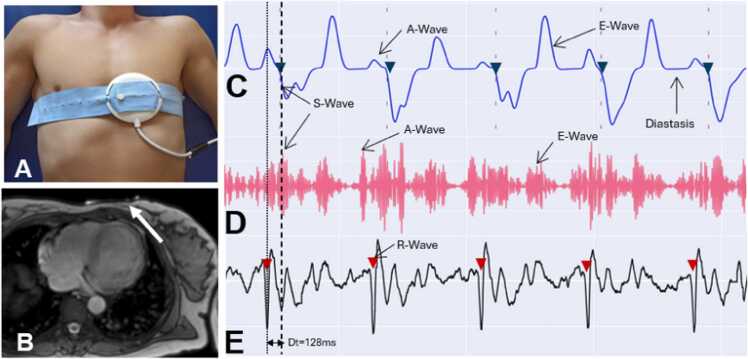
Background: Despite being a common gating method for cardiovascular magnetic resonance (CMR), electrocardiogram (ECG) gating has its disadvantages, and new gating strategies are desirable. An alternative CMR gating method is Doppler ultrasound (DUS) gating, which detects blood flow and ventricular movement. The aim of this study was to prove the feasibility of DUS gating as a novel CMR gating method in a clinical patient population.
Methods: In this prospective study, patients underwent clinically indicated CMR. Balanced steady-state free precession two-dimensional cine sequences in short-axis and 4-chamber views were acquired using ECG and DUS gating. DUS and ECG signal were recorded simultaneously. Time difference between R-wave and DUS systolic trigger detection was defined as trigger delay, the standard deviation of trigger delays as trigger jitter. Left and right ventricular parameters were assessed: left and right ventricular ejection fraction (LVEF, RVEF) and left and right ventricular end-diastolic volume index (LVEDVI, RVEDVI). Overall image quality was assessed using a 5-point Likert scale (5 = excellent to 1 = non-diagnostic). For statistical analysis, paired t-test, Wilcoxon test, Pearson correlation, and intraclass correlation coefficient (ICC) were employed.
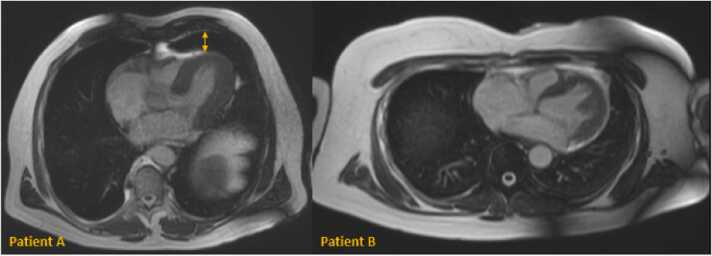
Results: Twenty-one patients (7 female) were included (age: 45.4 ± 19.7 years; body mass index: 27.6 ± 5.5 kg/m2). DUS mean trigger delay was 128 ± 28 ms. DUS mean trigger jitter was 23 ± 13 ms. Overall image quality showed no difference between ECG and DUS gating (e.g., short axis: 5 [interquartile range (IQR) 3-5] vs 4 [IQR 3.5-5]; P = 0.21). Quantitative analysis revealed no differences between ECG and DUS gating: LVEF (53.2 ± 9.2% vs 52.3 ± 9.1%; P = 0.18; ICC 0.97 [95% confidence interval [CI] 0.93-0.99]), LVEDVI (84.5 ± 15.8 mL/m2 vs 83.3 ± 15.8 mL/m2; P = 0.06; ICC 0.99 [95% CI 0.98-1.00]), RVEF (52.8 ± 8.0% vs 51.6 ± 7.2%; P = 0.06; ICC 0.96 [95% CI 0.89-0.99]), and RVEDVI (80.8 ± 17.6 mL/m2 vs 80.9 ± 16.5 mL/m2; P = 0.91; ICC 0.98 [95% CI 0.96-0.99]). In one patient with a prominent lingula of the lung image quality was non-diagnostic with DUS gating.
Conclusion: CMR gating with DUS is feasible and can offer an equivalent performance to ECG regarding image quality and quantitative parameter assessment.
期刊介绍:
Journal of Cardiovascular Magnetic Resonance (JCMR) publishes high-quality articles on all aspects of basic, translational and clinical research on the design, development, manufacture, and evaluation of cardiovascular magnetic resonance (CMR) methods applied to the cardiovascular system. Topical areas include, but are not limited to:
New applications of magnetic resonance to improve the diagnostic strategies, risk stratification, characterization and management of diseases affecting the cardiovascular system.
New methods to enhance or accelerate image acquisition and data analysis.
Results of multicenter, or larger single-center studies that provide insight into the utility of CMR.
Basic biological perceptions derived by CMR methods.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


