Mark L Urken, Margaret Brandwein-Weber, Raymond L Chai, Mark Zafereo, Maisie Shindo, Joseph Scharpf, Jun Fan, Alex Silberzweig, Justin K Joseph, Ronald Ghossein, Ashok Shaha, Zubair Baloch, R Michael Tuttle
{"title":"An anatomic checklist for accurate staging of grossly invasive thyroid cancer.","authors":"Mark L Urken, Margaret Brandwein-Weber, Raymond L Chai, Mark Zafereo, Maisie Shindo, Joseph Scharpf, Jun Fan, Alex Silberzweig, Justin K Joseph, Ronald Ghossein, Ashok Shaha, Zubair Baloch, R Michael Tuttle","doi":"10.1530/ETJ-24-0289","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The final surgical pathology report follows the patient throughout their cancer journey. For locoregionally advanced cancers, lack of surgeon-pathologist communication can lead to understaging, adversely impacting management. Our study aims to improve the accuracy of staging grossly invasive thyroid cancer by introducing an anatomic checklist, enhancing surgeon-pathologist communication.</p><p><strong>Methods: </strong>We studied 35 consecutive patients with either gross extrathyroidal or extranodal extension, 29 of whom underwent primary resections requiring AJCC staging. Surgeon A initially only dictated an operative report. Surgeon B transmitted an anatomic checklist to the pathologist in addition to the standard operative note. Final pathology reports were reviewed for AJCC staging accuracy. Surgeon A transitioned to submission of an anatomic checklist for his final six cases.</p><p><strong>Results: </strong>13 of the 14 final pathology reports without a checklist were understaged. All 15 cases with a surgeon completed anatomic checklist were accurately staged. There was a statistically significant improvement in the accuracy of staging reported in the final pathology reports when an anatomic checklist was submitted as compared to when it was not (P < 0.01, Fisher exact test, two-tailed). All final pathology reports for recurrent cases without a checklist failed to define the anatomic parts that were resected. The time to complete the checklist was less than 90 s.</p><p><strong>Conclusion: </strong>A surgeon-completed anatomic checklist allows pathologists to more accurately stage grossly invasive thyroid cancers. This rapidly completed form eliminates the need for pathologists to analyze the operative note and facilitates both risk of recurrence and AJCC stage determination.</p>","PeriodicalId":12159,"journal":{"name":"European Thyroid Journal","volume":" ","pages":""},"PeriodicalIF":4.3000,"publicationDate":"2025-03-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11896680/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Thyroid Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1530/ETJ-24-0289","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"Print","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The final surgical pathology report follows the patient throughout their cancer journey. For locoregionally advanced cancers, lack of surgeon-pathologist communication can lead to understaging, adversely impacting management. Our study aims to improve the accuracy of staging grossly invasive thyroid cancer by introducing an anatomic checklist, enhancing surgeon-pathologist communication.
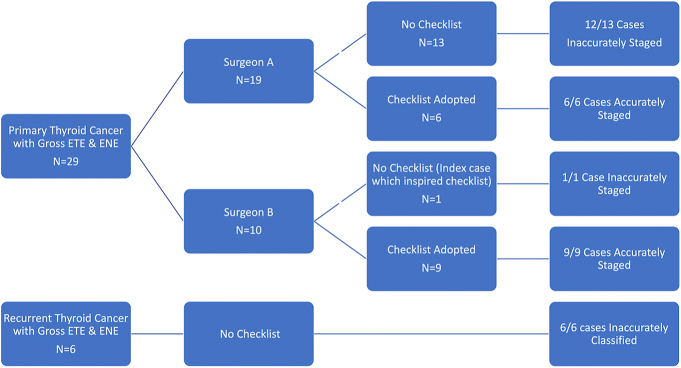
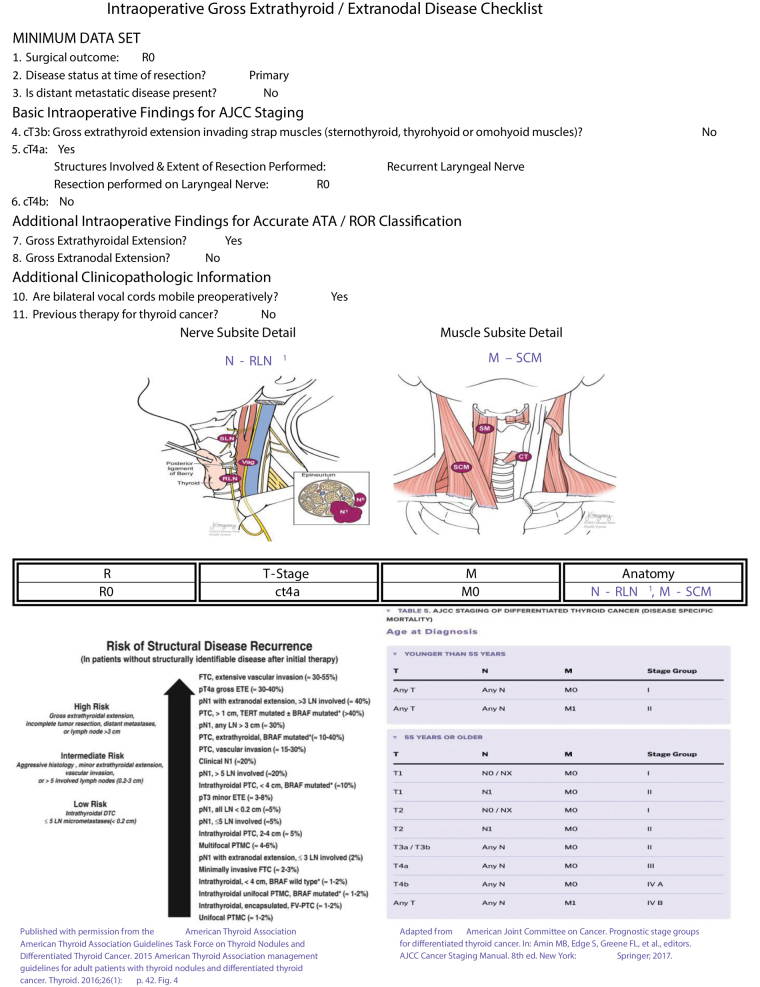
Methods: We studied 35 consecutive patients with either gross extrathyroidal or extranodal extension, 29 of whom underwent primary resections requiring AJCC staging. Surgeon A initially only dictated an operative report. Surgeon B transmitted an anatomic checklist to the pathologist in addition to the standard operative note. Final pathology reports were reviewed for AJCC staging accuracy. Surgeon A transitioned to submission of an anatomic checklist for his final six cases.
Results: 13 of the 14 final pathology reports without a checklist were understaged. All 15 cases with a surgeon completed anatomic checklist were accurately staged. There was a statistically significant improvement in the accuracy of staging reported in the final pathology reports when an anatomic checklist was submitted as compared to when it was not (P < 0.01, Fisher exact test, two-tailed). All final pathology reports for recurrent cases without a checklist failed to define the anatomic parts that were resected. The time to complete the checklist was less than 90 s.
Conclusion: A surgeon-completed anatomic checklist allows pathologists to more accurately stage grossly invasive thyroid cancers. This rapidly completed form eliminates the need for pathologists to analyze the operative note and facilitates both risk of recurrence and AJCC stage determination.
期刊介绍:
The ''European Thyroid Journal'' publishes papers reporting original research in basic, translational and clinical thyroidology. Original contributions cover all aspects of the field, from molecular and cellular biology to immunology and biochemistry, from physiology to pathology, and from pediatric to adult thyroid diseases with a special focus on thyroid cancer. Readers also benefit from reviews by noted experts, which highlight especially active areas of current research. The journal will further publish formal guidelines in the field, produced and endorsed by the European Thyroid Association.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


