Development of a predictive model for severe peripartum hemorrhage in placenta accreta spectrum cases under neuraxial anesthesia: a multicenter retrospective analysis.
{"title":"Development of a predictive model for severe peripartum hemorrhage in placenta accreta spectrum cases under neuraxial anesthesia: a multicenter retrospective analysis.","authors":"Yanan Li, Liang Li, Xiao Song, Fanqing Meng, Meiling Zhang, Yarong Li, Ran Chu","doi":"10.1177/26334941251317644","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The placenta accreta spectrum (PAS) represents a significant risk factor for severe postpartum hemorrhage. Recent studies have demonstrated the safety of neuraxial anesthesia (NA) in cesarean delivery (CD) for patients with PAS.</p><p><strong>Objectives: </strong>To evaluate the risk of severe peripartum hemorrhage in patients with PAS who underwent CD under NA.</p><p><strong>Design: </strong>A multicenter retrospective cohort study.</p><p><strong>Methods: </strong>This study analyzed 214 patients diagnosed with PAS. Logistic regression was used to identify factors increasing the risk of severe peripartum hemorrhage. A total of six machine learning (ML) algorithms were employed for model validation.</p><p><strong>Results: </strong>The predictive model includes the following risk factors: age at delivery >33 years (<i>p</i> = 0.004), history of CD >1 (<i>p</i> = 0.020), preoperative HGB ⩽ 100 g/L (<i>p</i> = 0.013), placenta previa classification (<i>p</i> = 0.001), vascular lacunae within the placenta (<i>p</i> = 0.015), and labor duration (<i>p</i> = 0.026). The validation of ML algorithms revealed that the model achieved an accuracy ranging from 0.68 to 0.71, with an area under the receiver operating characteristic curve between 0.75 and 0.79. A nomogram list and web-based calculator were constructed for clinical implementation, and a risk stratification system was established based on model scores.</p><p><strong>Conclusion: </strong>A prenatal risk assessment model was developed to estimate the likelihood of severe peripartum hemorrhage in PAS patients undergoing CD under NA. This model may provide preliminary support for clinicians in tailoring anesthetic management strategies for potentially high-risk cases, but further studies are needed to confirm its clinical utility.</p>","PeriodicalId":75219,"journal":{"name":"Therapeutic advances in reproductive health","volume":"19 ","pages":"26334941251317644"},"PeriodicalIF":1.8000,"publicationDate":"2025-02-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11815799/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic advances in reproductive health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26334941251317644","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The placenta accreta spectrum (PAS) represents a significant risk factor for severe postpartum hemorrhage. Recent studies have demonstrated the safety of neuraxial anesthesia (NA) in cesarean delivery (CD) for patients with PAS.
Objectives: To evaluate the risk of severe peripartum hemorrhage in patients with PAS who underwent CD under NA.
Design: A multicenter retrospective cohort study.
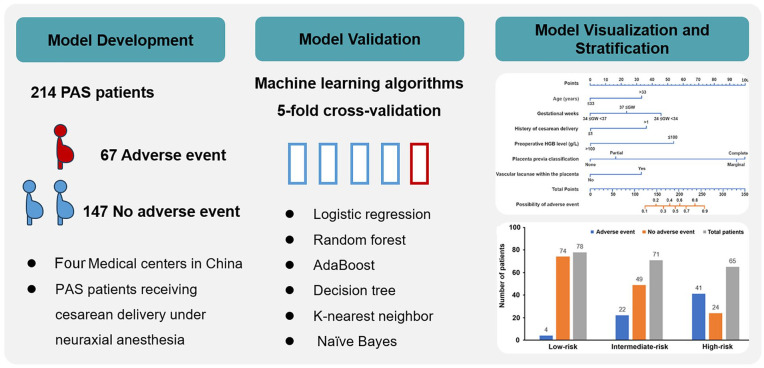
Methods: This study analyzed 214 patients diagnosed with PAS. Logistic regression was used to identify factors increasing the risk of severe peripartum hemorrhage. A total of six machine learning (ML) algorithms were employed for model validation.
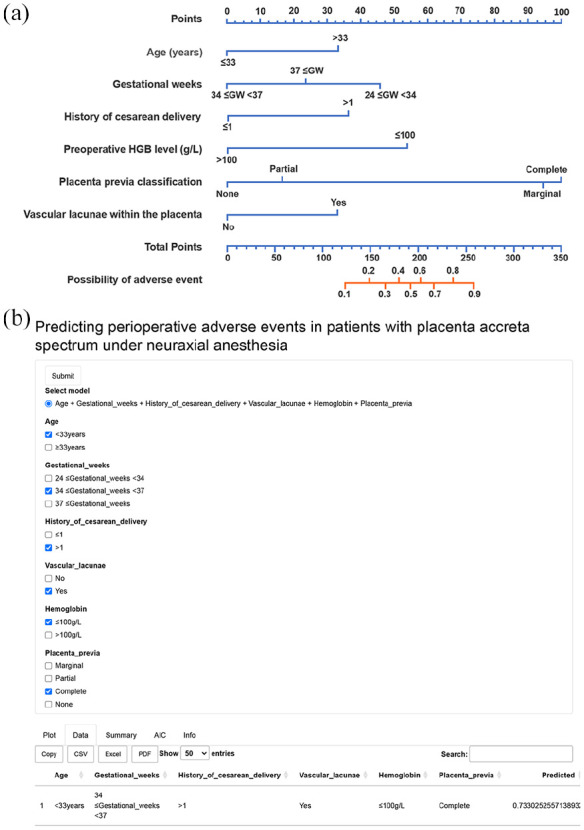
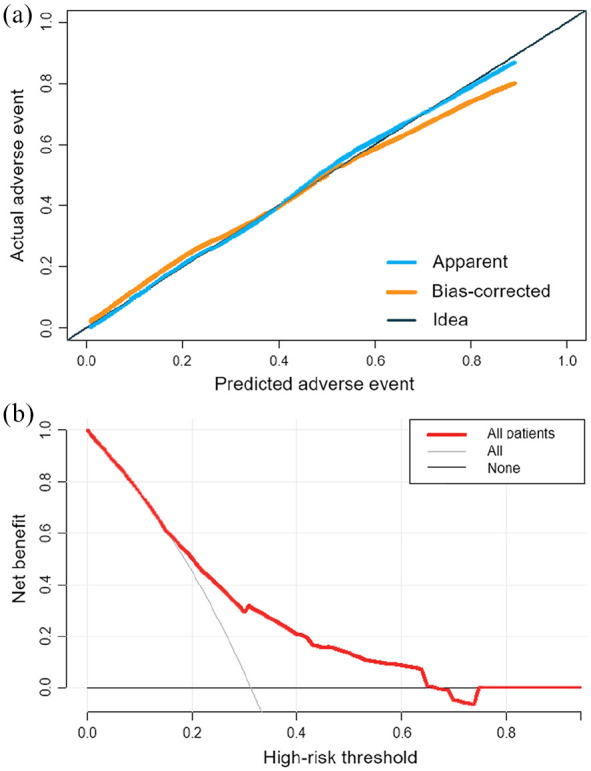
Results: The predictive model includes the following risk factors: age at delivery >33 years (p = 0.004), history of CD >1 (p = 0.020), preoperative HGB ⩽ 100 g/L (p = 0.013), placenta previa classification (p = 0.001), vascular lacunae within the placenta (p = 0.015), and labor duration (p = 0.026). The validation of ML algorithms revealed that the model achieved an accuracy ranging from 0.68 to 0.71, with an area under the receiver operating characteristic curve between 0.75 and 0.79. A nomogram list and web-based calculator were constructed for clinical implementation, and a risk stratification system was established based on model scores.
Conclusion: A prenatal risk assessment model was developed to estimate the likelihood of severe peripartum hemorrhage in PAS patients undergoing CD under NA. This model may provide preliminary support for clinicians in tailoring anesthetic management strategies for potentially high-risk cases, but further studies are needed to confirm its clinical utility.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


