Atypical Delayed-Onset Endophthalmitis Following Intravitreal Dexamethasone Implant Managed Without Implant Removal: A Rare Case Report and Literature Review.
{"title":"Atypical Delayed-Onset Endophthalmitis Following Intravitreal Dexamethasone Implant Managed Without Implant Removal: A Rare Case Report and Literature Review.","authors":"Amit Nandan Tripathi, Vipin Rana, Sandepan Bandopadhyay, Jaya Kaushik, Pradeep Kumar","doi":"10.22336/rjo.2024.64","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To report a case of atypical delayed-onset endophthalmitis following intravitreal dexamethasone (DEX) implantation, managed successfully without implant removal.</p><p><strong>Case presentation: </strong>A 72-year-old Asian woman with recurrent macular edema due to central retinal vein occlusion (CRVO) received an intravitreal DEX implant. Two weeks post-injection, she experienced blurred vision but no pain or redness. Best-corrected visual acuity (BCVA) had dropped to hand movements near the face (HMCF). Examination revealed 3+ anterior chamber cells and a 1.5 mm hypopyon, with significant vitreous haze obscuring retinal details. A diagnosis of acute endophthalmitis was made. Initial treatment with intravitreal vancomycin and ceftazidime was followed by pars plana vitrectomy (PPV) without implant removal. Microbiological tests were negative, and vision improved significantly, with BCVA returning to 6/12 after two weeks.</p><p><strong>Discussion: </strong>Endophthalmitis following DEX implantation is rare, and its management is not well-defined. While implant removal is often recommended, favorable outcomes can be achieved without it. The negative culture results and atypical presentation suggested a possible non-infectious etiology. Intraocular steroids may obscure typical signs of infection.</p><p><strong>Conclusion: </strong>Atypical delayed-onset endophthalmitis following DEX implantation can be successfully treated with prompt vitrectomy and intravitreal antibiotics without implant removal, underscoring the need for individualized management in such cases.</p>","PeriodicalId":94355,"journal":{"name":"Romanian journal of ophthalmology","volume":"68 4","pages":"343-348"},"PeriodicalIF":0.0000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11809834/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Romanian journal of ophthalmology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22336/rjo.2024.64","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To report a case of atypical delayed-onset endophthalmitis following intravitreal dexamethasone (DEX) implantation, managed successfully without implant removal.
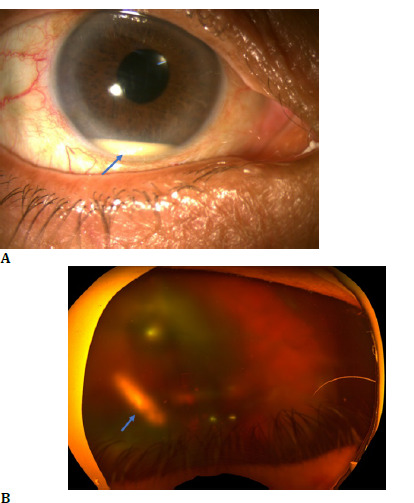
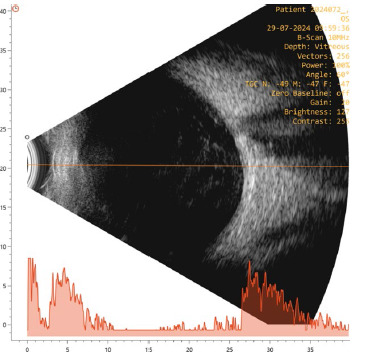
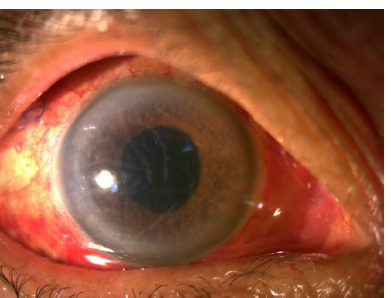
Case presentation: A 72-year-old Asian woman with recurrent macular edema due to central retinal vein occlusion (CRVO) received an intravitreal DEX implant. Two weeks post-injection, she experienced blurred vision but no pain or redness. Best-corrected visual acuity (BCVA) had dropped to hand movements near the face (HMCF). Examination revealed 3+ anterior chamber cells and a 1.5 mm hypopyon, with significant vitreous haze obscuring retinal details. A diagnosis of acute endophthalmitis was made. Initial treatment with intravitreal vancomycin and ceftazidime was followed by pars plana vitrectomy (PPV) without implant removal. Microbiological tests were negative, and vision improved significantly, with BCVA returning to 6/12 after two weeks.
Discussion: Endophthalmitis following DEX implantation is rare, and its management is not well-defined. While implant removal is often recommended, favorable outcomes can be achieved without it. The negative culture results and atypical presentation suggested a possible non-infectious etiology. Intraocular steroids may obscure typical signs of infection.
Conclusion: Atypical delayed-onset endophthalmitis following DEX implantation can be successfully treated with prompt vitrectomy and intravitreal antibiotics without implant removal, underscoring the need for individualized management in such cases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


