Francesco Marampon, Giovanni Luca Gravina, Elisa Cinelli, Lucy Zaccaro, Miriam Tomaciello, Nunzia Di Meglio, Francesco Gentili, Alfonso Cerase, Armando Perrella, Mariya Yavorska, Sami Aburas, Luciano Mutti, Maria Antonietta Mazzei, Giuseppe Minniti, Paolo Tini
{"title":"Reducing clinical target volume margins for multifocal glioblastoma: a multi-institutional analysis of patterns of recurrence and treatment response.","authors":"Francesco Marampon, Giovanni Luca Gravina, Elisa Cinelli, Lucy Zaccaro, Miriam Tomaciello, Nunzia Di Meglio, Francesco Gentili, Alfonso Cerase, Armando Perrella, Mariya Yavorska, Sami Aburas, Luciano Mutti, Maria Antonietta Mazzei, Giuseppe Minniti, Paolo Tini","doi":"10.3857/roj.2024.00059","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>No guidelines exist to delineate radiation therapy (RT) targets for the treatment of multiple glioblastoma (mGBM). This study analyzes margins around the gross tumor volume (GTV) to create a clinical target volume (CTV), comparing response parameters and modalities of recurrence. Material and Methods: One-hundred and three mGBM patients with a CTV margin of 2 cm (GTV + 2.0 cm) or 1 cm (GTV + 1.0 cm) were retrospectively analyzed. All patients received a total dose of 59.4-60 Gy in 1.8-2.0 Gy daily fractions, delivered from 4 to 8 weeks after surgery, concomitantly with temozolomide (75 mg/m2). Overall survival (OS) and progression-free survival (PFS) were calculated from the date of surgery until diagnosis of disease progression performed by magnetic resonance imaging and classified as marginal, in-field, or distant, comparing site of progression with dose distribution in RT plan.</p><p><strong>Results: </strong>OS in mGBM CTV1 group was 11.2 months (95% confidence interval [CI], 10.3-12.1), and 9.2 months in mGBM CTV2 group (95% CI, 9.0-11.3). PFS in mGBM CTV1 group occurred within 8.3 months (95% CI, 7.3-9.3), and 7.3 months in mGBM CTV2 group (95% CI, 6.4-8.1). No difference was observed between the two groups in terms of OS and PFS time distribution. Adjusted to a multivariate Cox risk model, epidermal growth factor receptor amplification resulted a negative prognostic factor for both OS and PFS.</p><p><strong>Conclusion: </strong>In mGBM, the use of a 1 cm CTV expansion seems feasible as it does not significantly affect oncological outcomes and progression outcome.</p>","PeriodicalId":94184,"journal":{"name":"Radiation oncology journal","volume":" ","pages":"13-21"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12010890/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation oncology journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3857/roj.2024.00059","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/19 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
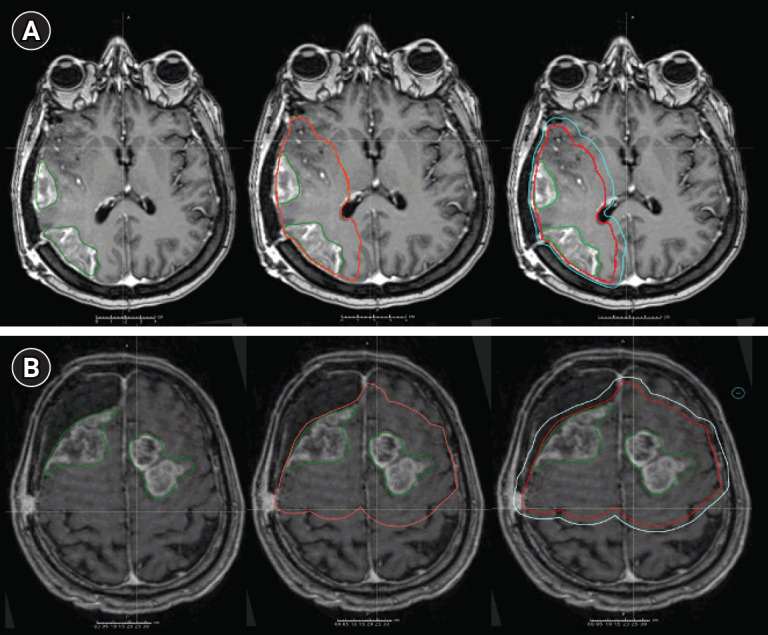
Purpose: No guidelines exist to delineate radiation therapy (RT) targets for the treatment of multiple glioblastoma (mGBM). This study analyzes margins around the gross tumor volume (GTV) to create a clinical target volume (CTV), comparing response parameters and modalities of recurrence. Material and Methods: One-hundred and three mGBM patients with a CTV margin of 2 cm (GTV + 2.0 cm) or 1 cm (GTV + 1.0 cm) were retrospectively analyzed. All patients received a total dose of 59.4-60 Gy in 1.8-2.0 Gy daily fractions, delivered from 4 to 8 weeks after surgery, concomitantly with temozolomide (75 mg/m2). Overall survival (OS) and progression-free survival (PFS) were calculated from the date of surgery until diagnosis of disease progression performed by magnetic resonance imaging and classified as marginal, in-field, or distant, comparing site of progression with dose distribution in RT plan.
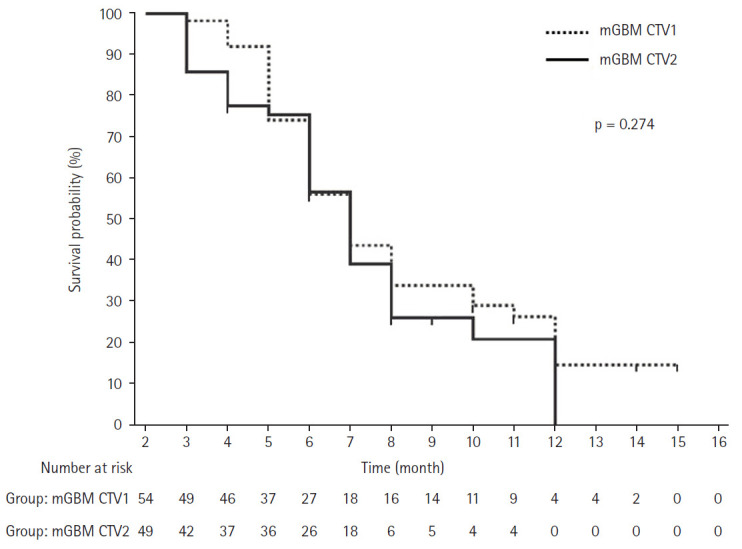
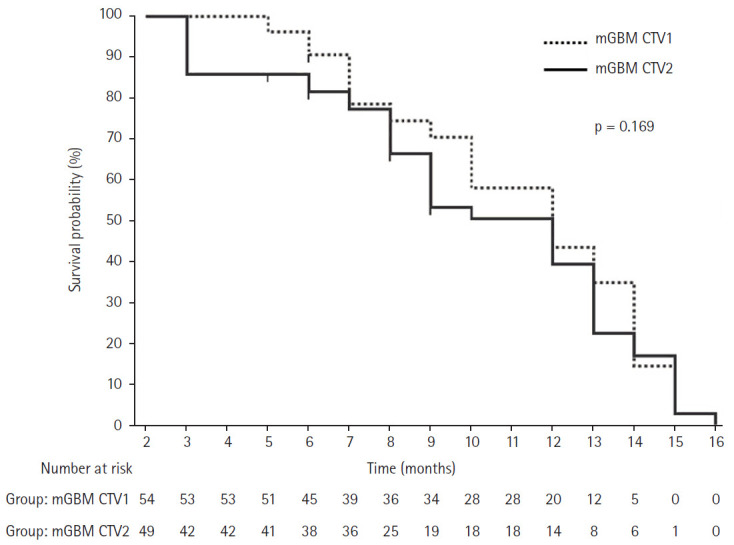
Results: OS in mGBM CTV1 group was 11.2 months (95% confidence interval [CI], 10.3-12.1), and 9.2 months in mGBM CTV2 group (95% CI, 9.0-11.3). PFS in mGBM CTV1 group occurred within 8.3 months (95% CI, 7.3-9.3), and 7.3 months in mGBM CTV2 group (95% CI, 6.4-8.1). No difference was observed between the two groups in terms of OS and PFS time distribution. Adjusted to a multivariate Cox risk model, epidermal growth factor receptor amplification resulted a negative prognostic factor for both OS and PFS.
Conclusion: In mGBM, the use of a 1 cm CTV expansion seems feasible as it does not significantly affect oncological outcomes and progression outcome.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


