Caitlyn F. Connor, Jesse Riker, Laura K. Burns, Jörg Mayer, Jesse M. Hostetter, Katie Metcalf
{"title":"What is your diagnosis? Fine-needle aspirate from a subcutaneous preputial mass in a ferret","authors":"Caitlyn F. Connor, Jesse Riker, Laura K. Burns, Jörg Mayer, Jesse M. Hostetter, Katie Metcalf","doi":"10.1111/vcp.13414","DOIUrl":null,"url":null,"abstract":"<p>A 3-year-old castrated male ferret was evaluated for several months' history of alopecia and a more recent history of lethargy, inappetence, and stranguria. Physical examination revealed splenomegaly and an approximately 1 cm freely movable, firm, raised, purple, subcutaneous mass on the prepuce.</p><p>A CBC revealed a severe normocytic, normochromic anemia (ADVIA 2120, HCT 17.5%, RI: 40–51%) consistent with anemia of inflammation; however, given the severity, other components such as occult bleeding causing a pre-regenerative anemia were suspected. Additionally, there was an inflammatory leukogram with a stress component characterized by a moderate leukocytosis (WBC 31.4 × 10<sup>3</sup>/μL, RI: 2.7–11.2 × 10<sup>3</sup>/μL) with a moderate, mature neutrophilia (29.516 × 10<sup>3</sup>/μL, RI: 1.0–8.0 × 10<sup>3</sup>/μL), mild monocytosis (1.256 × 10<sup>3</sup>/μL, RI: 0.0–0.9 × 10<sup>3</sup>/μL), and a mild lymphopenia (0.628 × 10<sup>3</sup>/μL, RI: 1.0–6.3 × 10<sup>3</sup>/μL).<span><sup>1</sup></span> A blood gas analysis (Nova) revealed no significant abnormalities. Prior to referral, an adrenal panel revealed moderate elevations in progesterone (1.24 nmol/L, RI: <0.1–0.80) and estradiol concentrations within the reference interval, supportive of adrenal disease.</p><p>Abdominal ultrasound revealed several abnormalities, including a heterogeneous, cavitated gastric mass, abdominal lymphadenopathy, diffuse splenomegaly with splenic nodules, a right adrenal nodule, and scant peritoneal effusion. Aspirates of the preputial mass (Figure 1), as well as ultrasound-guided fine-needle aspirates of the spleen and gastric mass, were submitted for cytologic evaluation. Splenic aspirates revealed a heterogeneous lymphoid population with many erythroid and myeloid precursors, consistent with a reactive spleen with marked extramedullary hematopoiesis. The gastric mass aspirate smears revealed marked, septic, neutrophilic inflammation with moderate lymphocytic infiltrate.</p><p>Malignant neoplasm, consistent with apocrine gland adenocarcinoma with moderate neutrophilic inflammation and hemorrhage.</p><p>Smears exhibited excellent cellularity with abundant individualized to clustered pleomorphic cells found in palisading, acinar, or crowded arrangements (Figure 1A,B). These cells were variably shaped (polygonal, cuboidal, columnar, to rarely spindled) with moderate amounts of pale basophilic cytoplasm that often contained few dark blue-green secretory granules or eosinophilic globules (Figure 1C,D). Nuclei were round to ovoid and centrally placed, with coarsely stippled chromatin and 1–3 distinct round nucleoli. Cells demonstrated moderate anisocytosis and anisokaryosis, frequent binucleation, and rare multinucleation (up to 4 nuclei) with nuclear molding. Small amounts of extracellular, pale eosinophilic material were seen associated with these cell clusters. Moderate numbers of variably degenerate neutrophils and few vacuolated macrophages exhibiting erythrophagia were also present.</p><p>Given the concerning ultrasound and cytology findings, exploratory laparotomy was pursued. During surgery, three nodules were also observed on the pancreas. A splenectomy, partial pancreatectomy, partial gastrectomy, and preputial mass excision were performed. Histopathology revealed an unencapsulated, well-defined, highly cellular preputial mass that expanded and replaced the deep dermis (Figure 2A). Neoplastic cells were arranged in tubuloacini and cords amidst a thin fibrovascular stroma (Figure 2B). The tubuloacini occasionally contained varying amounts of brightly eosinophilic, homogenous, acellular material and/or neutrophils. The neoplastic cells were polygonal to cuboidal with well-defined cell borders, moderate amounts of eosinophilic cytoplasm, and a primarily basilar, round to ovoid nucleus with sparse chromatin and 1–2 small, basophilic nucleoli. Within acini, cells had apical cytoplasmic blebbing (Figure 2C). There was mild anisocytosis and anisokaryosis, and the mitotic count was 4 per 2.37 mm<sup>2</sup> (equivalent to 10 FN22/40X fields). Neoplastic cells abutted the deep margins. The final diagnosis for the preputial mass was apocrine gland adenocarcinoma.</p><p>Additional histopathology results included mild neutrophilic pancreatitis with fibrosis as well as multifocal islet cell tumors (presumed insulinomas), chronic gastric abscessation, and splenic reactive lymphoid hyperplasia. Following recovery, the patient arrested, and resuscitation attempts were unsuccessful. A necropsy was not performed.</p><p>The most common neoplasms described in ferrets often involve the endocrine (pancreatic islets, adrenal cortex), integumentary, or hemolymphatic systems (ie, lymphoma).<span><sup>2, 3</sup></span> Regarding cutaneous neoplasms, apocrine gland neoplasms are the third most common, following basal cell tumors and mast cell tumors.<span><sup>3, 4</sup></span> Apocrine glands are scent glands that are present throughout the haired skin, with the highest concentrations of these glands present at the head, neck, prepuce, and vulva.<span><sup>2</sup></span> Apocrine glands within these areas share a similar function and do not have specialized forms based on anatomic location, such as those seen in the ear (e.g., ceruminous glands) and mammary glands.<span><sup>2, 5</sup></span> Given the higher concentrations of these glands, apocrine neoplasms are more commonly found in these locations compared with other areas of the body.<span><sup>6</sup></span></p><p>While benign apocrine neoplasms (adenomas and cystadenomas) are documented, when specifically associated with the prepuce or vulvar regions, apocrine gland neoplasms in the ferret are more frequently malignant (up to 75% of preputial apocrine neoplasms), exhibiting aggressive local tissue invasion, a higher incidence of recurrence following surgical excision, and frequent metastasis to regional lymph nodes.<span><sup>2-4</sup></span> These tumors are described as large, firm, variably mobile masses that are often pigmented, appearing purple to black.<span><sup>2</sup></span> Current treatment recommendations include wide surgical excision with palliative radiation therapy; however, given the aggressive behavior, these tumors carry a poor prognosis.<span><sup>3, 6</sup></span> Without a necropsy, the significance of this patient's apocrine adenocarcinoma and the post-operative arrest cannot be ascertained.</p><p>The cytologic features (blue-green globular intracytoplasmic material) of the apocrine adenocarcinoma, in this case, are akin to what has been previously observed.<span><sup>7</sup></span> However, the presence of eosinophilic granules within the cytoplasm of these cells has not been previously described to the authors' knowledge. Studies of human apocrine cells note two distinct cytoplasmic granules/bodies with transmission electron microscopy.<span><sup>8</sup></span> The correlation between the presence or absence of these granules observed cytologically and the biological behavior of these tumors has not been evaluated. The described blue-green granules were not observed in the case by Pinches et al, whereas this case contained granules similar to those of Rakich et al with the addition of eosinophilic granular material. It would be interesting to investigate if this cytologic discrepancy provides any further predictive information on tumor behavior. In concordance with other reports, this case also exhibited eosinophilic extracellular material often in the background or adjacent to the clusters of neoplastic cells<span><sup>5, 7</sup></span> This material may represent basement membrane, collagenous matrix, or, similar to Pinches et al, represent secretory material. These findings support the glandular origin of these neoplasms, given the presence of intracellular material and occasional acinar arrangements of the epithelial cells. Other differentials for neoplasms in this area with similar cytomorphology include mammary epithelial neoplasms or metastatic adenocarcinomas of cutaneous or non-cutaneous origin.</p><p>This case demonstrates the cytologic and histologic findings of an apocrine adenocarcinoma on the prepuce of a ferret and highlights the subtle variations in the cytomorphology that exist for these neoplasms, further adding to the case index for this tumor type.</p><p>The authors have indicated that they have no affiliations or financial involvement with any organization or entity with a financial interest in, or in financial competition with, the subject matter or materials discussed in this article.</p>","PeriodicalId":23593,"journal":{"name":"Veterinary clinical pathology","volume":"54 S1","pages":"S60-S63"},"PeriodicalIF":1.1000,"publicationDate":"2025-02-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/vcp.13414","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Veterinary clinical pathology","FirstCategoryId":"97","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/vcp.13414","RegionNum":4,"RegionCategory":"农林科学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"VETERINARY SCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
A 3-year-old castrated male ferret was evaluated for several months' history of alopecia and a more recent history of lethargy, inappetence, and stranguria. Physical examination revealed splenomegaly and an approximately 1 cm freely movable, firm, raised, purple, subcutaneous mass on the prepuce.
A CBC revealed a severe normocytic, normochromic anemia (ADVIA 2120, HCT 17.5%, RI: 40–51%) consistent with anemia of inflammation; however, given the severity, other components such as occult bleeding causing a pre-regenerative anemia were suspected. Additionally, there was an inflammatory leukogram with a stress component characterized by a moderate leukocytosis (WBC 31.4 × 103/μL, RI: 2.7–11.2 × 103/μL) with a moderate, mature neutrophilia (29.516 × 103/μL, RI: 1.0–8.0 × 103/μL), mild monocytosis (1.256 × 103/μL, RI: 0.0–0.9 × 103/μL), and a mild lymphopenia (0.628 × 103/μL, RI: 1.0–6.3 × 103/μL).1 A blood gas analysis (Nova) revealed no significant abnormalities. Prior to referral, an adrenal panel revealed moderate elevations in progesterone (1.24 nmol/L, RI: <0.1–0.80) and estradiol concentrations within the reference interval, supportive of adrenal disease.
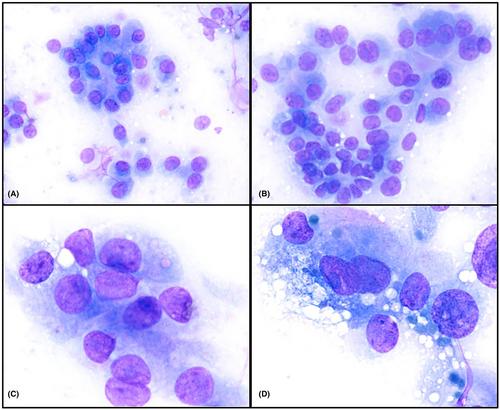
Abdominal ultrasound revealed several abnormalities, including a heterogeneous, cavitated gastric mass, abdominal lymphadenopathy, diffuse splenomegaly with splenic nodules, a right adrenal nodule, and scant peritoneal effusion. Aspirates of the preputial mass (Figure 1), as well as ultrasound-guided fine-needle aspirates of the spleen and gastric mass, were submitted for cytologic evaluation. Splenic aspirates revealed a heterogeneous lymphoid population with many erythroid and myeloid precursors, consistent with a reactive spleen with marked extramedullary hematopoiesis. The gastric mass aspirate smears revealed marked, septic, neutrophilic inflammation with moderate lymphocytic infiltrate.
Malignant neoplasm, consistent with apocrine gland adenocarcinoma with moderate neutrophilic inflammation and hemorrhage.
Smears exhibited excellent cellularity with abundant individualized to clustered pleomorphic cells found in palisading, acinar, or crowded arrangements (Figure 1A,B). These cells were variably shaped (polygonal, cuboidal, columnar, to rarely spindled) with moderate amounts of pale basophilic cytoplasm that often contained few dark blue-green secretory granules or eosinophilic globules (Figure 1C,D). Nuclei were round to ovoid and centrally placed, with coarsely stippled chromatin and 1–3 distinct round nucleoli. Cells demonstrated moderate anisocytosis and anisokaryosis, frequent binucleation, and rare multinucleation (up to 4 nuclei) with nuclear molding. Small amounts of extracellular, pale eosinophilic material were seen associated with these cell clusters. Moderate numbers of variably degenerate neutrophils and few vacuolated macrophages exhibiting erythrophagia were also present.
Given the concerning ultrasound and cytology findings, exploratory laparotomy was pursued. During surgery, three nodules were also observed on the pancreas. A splenectomy, partial pancreatectomy, partial gastrectomy, and preputial mass excision were performed. Histopathology revealed an unencapsulated, well-defined, highly cellular preputial mass that expanded and replaced the deep dermis (Figure 2A). Neoplastic cells were arranged in tubuloacini and cords amidst a thin fibrovascular stroma (Figure 2B). The tubuloacini occasionally contained varying amounts of brightly eosinophilic, homogenous, acellular material and/or neutrophils. The neoplastic cells were polygonal to cuboidal with well-defined cell borders, moderate amounts of eosinophilic cytoplasm, and a primarily basilar, round to ovoid nucleus with sparse chromatin and 1–2 small, basophilic nucleoli. Within acini, cells had apical cytoplasmic blebbing (Figure 2C). There was mild anisocytosis and anisokaryosis, and the mitotic count was 4 per 2.37 mm2 (equivalent to 10 FN22/40X fields). Neoplastic cells abutted the deep margins. The final diagnosis for the preputial mass was apocrine gland adenocarcinoma.
Additional histopathology results included mild neutrophilic pancreatitis with fibrosis as well as multifocal islet cell tumors (presumed insulinomas), chronic gastric abscessation, and splenic reactive lymphoid hyperplasia. Following recovery, the patient arrested, and resuscitation attempts were unsuccessful. A necropsy was not performed.
The most common neoplasms described in ferrets often involve the endocrine (pancreatic islets, adrenal cortex), integumentary, or hemolymphatic systems (ie, lymphoma).2, 3 Regarding cutaneous neoplasms, apocrine gland neoplasms are the third most common, following basal cell tumors and mast cell tumors.3, 4 Apocrine glands are scent glands that are present throughout the haired skin, with the highest concentrations of these glands present at the head, neck, prepuce, and vulva.2 Apocrine glands within these areas share a similar function and do not have specialized forms based on anatomic location, such as those seen in the ear (e.g., ceruminous glands) and mammary glands.2, 5 Given the higher concentrations of these glands, apocrine neoplasms are more commonly found in these locations compared with other areas of the body.6
While benign apocrine neoplasms (adenomas and cystadenomas) are documented, when specifically associated with the prepuce or vulvar regions, apocrine gland neoplasms in the ferret are more frequently malignant (up to 75% of preputial apocrine neoplasms), exhibiting aggressive local tissue invasion, a higher incidence of recurrence following surgical excision, and frequent metastasis to regional lymph nodes.2-4 These tumors are described as large, firm, variably mobile masses that are often pigmented, appearing purple to black.2 Current treatment recommendations include wide surgical excision with palliative radiation therapy; however, given the aggressive behavior, these tumors carry a poor prognosis.3, 6 Without a necropsy, the significance of this patient's apocrine adenocarcinoma and the post-operative arrest cannot be ascertained.
The cytologic features (blue-green globular intracytoplasmic material) of the apocrine adenocarcinoma, in this case, are akin to what has been previously observed.7 However, the presence of eosinophilic granules within the cytoplasm of these cells has not been previously described to the authors' knowledge. Studies of human apocrine cells note two distinct cytoplasmic granules/bodies with transmission electron microscopy.8 The correlation between the presence or absence of these granules observed cytologically and the biological behavior of these tumors has not been evaluated. The described blue-green granules were not observed in the case by Pinches et al, whereas this case contained granules similar to those of Rakich et al with the addition of eosinophilic granular material. It would be interesting to investigate if this cytologic discrepancy provides any further predictive information on tumor behavior. In concordance with other reports, this case also exhibited eosinophilic extracellular material often in the background or adjacent to the clusters of neoplastic cells5, 7 This material may represent basement membrane, collagenous matrix, or, similar to Pinches et al, represent secretory material. These findings support the glandular origin of these neoplasms, given the presence of intracellular material and occasional acinar arrangements of the epithelial cells. Other differentials for neoplasms in this area with similar cytomorphology include mammary epithelial neoplasms or metastatic adenocarcinomas of cutaneous or non-cutaneous origin.
This case demonstrates the cytologic and histologic findings of an apocrine adenocarcinoma on the prepuce of a ferret and highlights the subtle variations in the cytomorphology that exist for these neoplasms, further adding to the case index for this tumor type.
The authors have indicated that they have no affiliations or financial involvement with any organization or entity with a financial interest in, or in financial competition with, the subject matter or materials discussed in this article.
期刊介绍:
Veterinary Clinical Pathology is the official journal of the American Society for Veterinary Clinical Pathology (ASVCP) and the European Society of Veterinary Clinical Pathology (ESVCP). The journal''s mission is to provide an international forum for communication and discussion of scientific investigations and new developments that advance the art and science of laboratory diagnosis in animals. Veterinary Clinical Pathology welcomes original experimental research and clinical contributions involving domestic, laboratory, avian, and wildlife species in the areas of hematology, hemostasis, immunopathology, clinical chemistry, cytopathology, surgical pathology, toxicology, endocrinology, laboratory and analytical techniques, instrumentation, quality assurance, and clinical pathology education.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


