Biphasic anaphylaxis in a Canadian tertiary care centre: an evaluation of incidence and risk factors from electronic health records and telephone interviews.
Anne K Ellis, Lubnaa Hossenbaccus, Sophia Linton, Hannah Botting, Eman Badawod, Alyssa Burrows, Sarah Garvey
{"title":"Biphasic anaphylaxis in a Canadian tertiary care centre: an evaluation of incidence and risk factors from electronic health records and telephone interviews.","authors":"Anne K Ellis, Lubnaa Hossenbaccus, Sophia Linton, Hannah Botting, Eman Badawod, Alyssa Burrows, Sarah Garvey","doi":"10.1186/s13223-024-00919-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Our previous 2007 study reported a 19.4% rate of biphasic anaphylaxis in Kingston, Ontario. Since then, few updates have been published regarding the etiology and risk factors of biphasic anaphylaxis. This study aimed to describe the incidence of and predictors of biphasic anaphylaxis in a single centre through a retrospective evaluation of patients with diagnosed anaphylaxis.</p><p><strong>Methods: </strong>From November 2015 to August 2017, all patients who presented to the emergency department at two hospital sites in Kingston given a diagnosis of \"allergic reaction,\" \"anaphylaxis,\" \"drug allergy,\" or \"insect sting allergy,\" were evaluated. Patients were contacted sometime after ED discharge to obtain consent and confirm symptoms and timing of the reaction. A trained allergist determined if criteria for anaphylaxis were met and categorized the reactions as being uniphasic, biphasic, or non-anaphylactic biphasic. A full medical review of the event ensued, and each type of anaphylactic event was statistically compared.</p><p><strong>Results: </strong>Of 138 anaphylactic events identified, 15.94% were biphasic reactions, 79.0% were uniphasic, and 5.07% were classified alternatively as a non-anaphylactic biphasic reaction. The average time of a second reaction was 19.0 h in patients experiencing biphasic reactivity. For biphasic anaphylaxis, the symptom profiles of second reactions were significantly less severe (p = 0.0002) compared with the initial reaction but significantly more severe than non-anaphylactic biphasic events (p < 0.0001).No differences of management were identified between events.</p><p><strong>Conclusion: </strong>The incidence of biphasic reactions in this cohort was 15.94% and the average second-phase onset was 19.0 h. In biphasic reactivity, it appears that the symptom profile second reaction is less severe compared to the first reaction.</p>","PeriodicalId":51302,"journal":{"name":"Allergy Asthma and Clinical Immunology","volume":"21 1","pages":"7"},"PeriodicalIF":2.4000,"publicationDate":"2025-02-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11806842/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Allergy Asthma and Clinical Immunology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13223-024-00919-2","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Our previous 2007 study reported a 19.4% rate of biphasic anaphylaxis in Kingston, Ontario. Since then, few updates have been published regarding the etiology and risk factors of biphasic anaphylaxis. This study aimed to describe the incidence of and predictors of biphasic anaphylaxis in a single centre through a retrospective evaluation of patients with diagnosed anaphylaxis.
Methods: From November 2015 to August 2017, all patients who presented to the emergency department at two hospital sites in Kingston given a diagnosis of "allergic reaction," "anaphylaxis," "drug allergy," or "insect sting allergy," were evaluated. Patients were contacted sometime after ED discharge to obtain consent and confirm symptoms and timing of the reaction. A trained allergist determined if criteria for anaphylaxis were met and categorized the reactions as being uniphasic, biphasic, or non-anaphylactic biphasic. A full medical review of the event ensued, and each type of anaphylactic event was statistically compared.
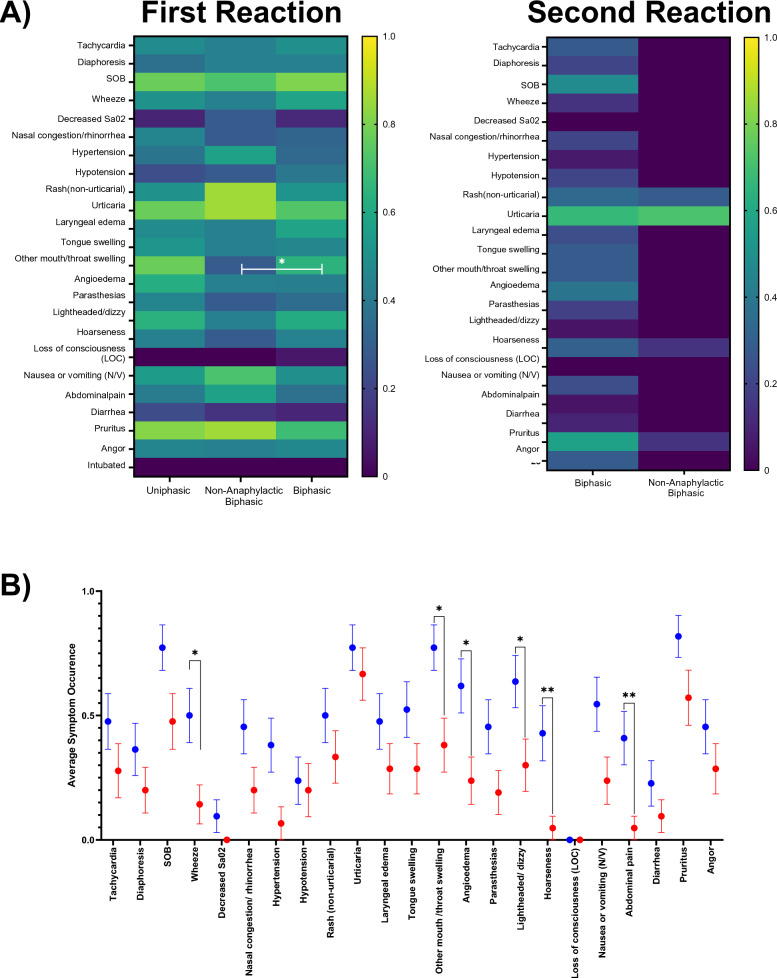
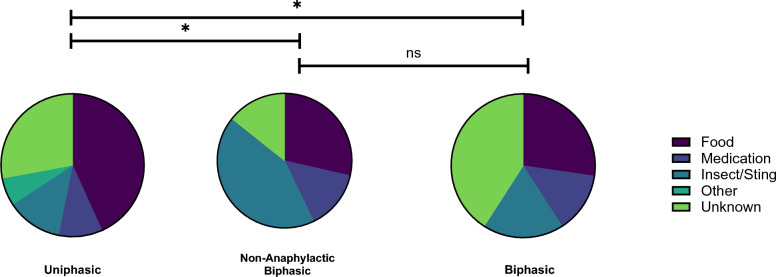
Results: Of 138 anaphylactic events identified, 15.94% were biphasic reactions, 79.0% were uniphasic, and 5.07% were classified alternatively as a non-anaphylactic biphasic reaction. The average time of a second reaction was 19.0 h in patients experiencing biphasic reactivity. For biphasic anaphylaxis, the symptom profiles of second reactions were significantly less severe (p = 0.0002) compared with the initial reaction but significantly more severe than non-anaphylactic biphasic events (p < 0.0001).No differences of management were identified between events.
Conclusion: The incidence of biphasic reactions in this cohort was 15.94% and the average second-phase onset was 19.0 h. In biphasic reactivity, it appears that the symptom profile second reaction is less severe compared to the first reaction.
期刊介绍:
Allergy, Asthma & Clinical Immunology (AACI), the official journal of the Canadian Society of Allergy and Clinical Immunology (CSACI), is an open access journal that encompasses all aspects of diagnosis, epidemiology, prevention and treatment of allergic and immunologic disease.
By offering a high-visibility forum for new insights and discussions, AACI provides a platform for the dissemination of allergy and clinical immunology research and reviews amongst allergists, pulmonologists, immunologists and other physicians, healthcare workers, medical students and the public worldwide.
AACI reports on basic research and clinically applied studies in the following areas and other related topics: asthma and occupational lung disease, rhinoconjunctivitis and rhinosinusitis, drug hypersensitivity, allergic skin diseases, urticaria and angioedema, venom hypersensitivity, anaphylaxis and food allergy, immunotherapy, immune modulators and biologics, immune deficiency and autoimmunity, T cell and B cell functions, regulatory T cells, natural killer cells, mast cell and eosinophil functions, complement abnormalities.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


