{"title":"Identification of the optimal candidates to benefit from surgery and chemotherapy among elderly female breast cancer patients with bone metastases.","authors":"Yuchen Hu, Junfeng Tang, Xiaofeng Liu, Yusheng Sun, Baojun Gong, Qing Gao","doi":"10.1038/s41598-025-89222-7","DOIUrl":null,"url":null,"abstract":"<p><p>Breast cancer is currently the most common malignant tumor affecting women's health worldwide. The rise in breast cancer metastases among patients is attributed to the inherent variability in metastatic behavior. In breast cancer, bones are the primary location for distant metastases, significantly impacting the survival rates of elderly (≥ 65) patients. The use of surgery and chemotherapy in this population is controversial. This study seeks to create a tool for forecasting overall survival (OS) in older breast cancer patients with bone metastases and to determine the optimal candidates for surgery and chemotherapy. Elderly female breast cancer patients with bone metastases from the Surveillance, Epidemiology, and End Results (SEER) database were included in this study and categorized into a training cohort and a validation cohort using R software. To identify independent predictors of OS in this population, both univariate and multivariate Cox regression analyses were conducted. Subsequently, a prognostic nomogram was created to estimate OS at 12, 24, and 36 months. The nomogram's accuracy and practical value were assessed using a calibration curve, area under the curve (AUC), and decision curve analysis (DCA). At the same time, a mortality risk classification system based on the nomogram was created to divide the population into high and low mortality risk categories, and subgroups were analyzed to determine the optimal candidates for surgery and chemotherapy. This study encompassed 2257 elderly female breast cancer patients with bone metastases, divided into 1581 participants for the training cohort and 676 for the validation cohort. Both univariate and multivariate Cox regression analyses validated those variables such as age, race, marital status, histological type, tumor grade, ER status, PR status, breast subtype, distant metastases (lung, liver, and brain), and treatment methods (surgery and chemotherapy) independently predicted OS in elderly female breast cancer patients with bone metastases (p < 0.05). Utilizing these independent predictors, a prognostic nomogram was developed to estimate OS at 12, 24, and 36 months. The calibration curves indicated that the nomogram's predictions closely matched the observed outcomes. The nomogram's AUC for forecasting OS at 12, 24, and 36 months was 0.753, 0.748, and 0.745 in the training cohort, and 0.744, 0.723, and 0.723 in the validation cohort. Additionally, the nomogram's AUC surpassed that of any individual independent predictor. DCA showed that the nomogram could achieve more net clinical benefit over a broader range of threshold probabilities. The nomogram-based risk classification system effectively sorted patients into two categories: low risk (≤ 820) and high risk (> 820). Subgroup analysis indicated that individuals classified as low-risk experienced the greatest advantage from surgery and chemotherapy (p < 0.05), whereas the high-risk group did not exhibit a statistically significant difference (p > 0.05). Drawing from the clinicopathological characteristics of elderly female breast cancer patients with bone metastases, this study developed a novel prognostic nomogram to forecast OS at 12, 24, and 36 months, enabling precise survival predictions. In addition, this study also constructed a mortality risk classification system, which can effectively help clinicians screen out the optimal candidates to benefit from surgery and chemotherapy and rationalize the allocation of medical resources.</p>","PeriodicalId":21811,"journal":{"name":"Scientific Reports","volume":"15 1","pages":"4678"},"PeriodicalIF":3.9000,"publicationDate":"2025-02-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11806091/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scientific Reports","FirstCategoryId":"103","ListUrlMain":"https://doi.org/10.1038/s41598-025-89222-7","RegionNum":2,"RegionCategory":"综合性期刊","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MULTIDISCIPLINARY SCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
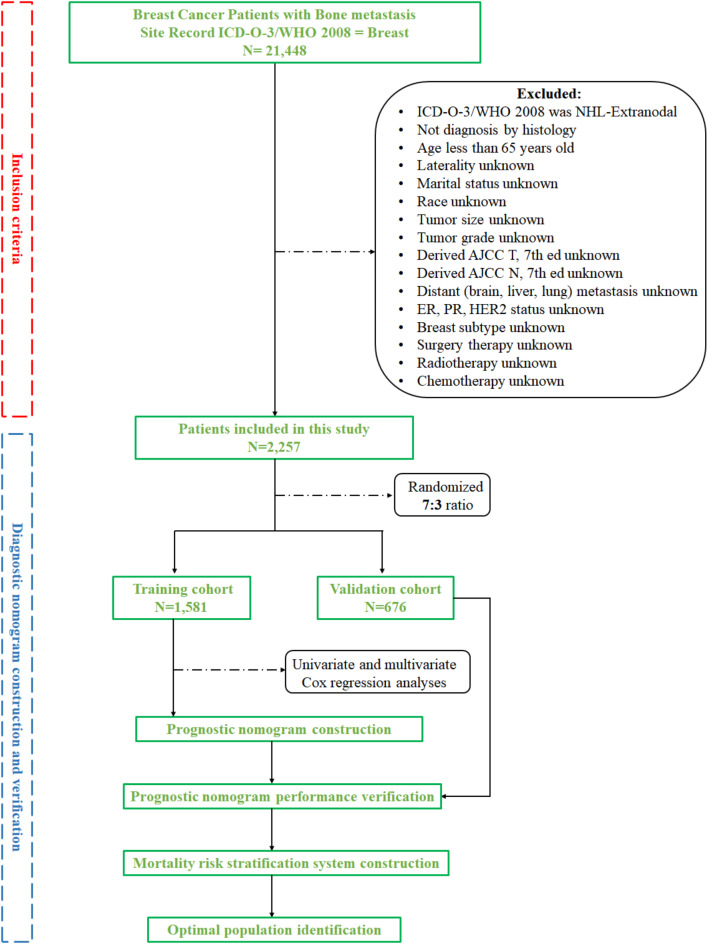
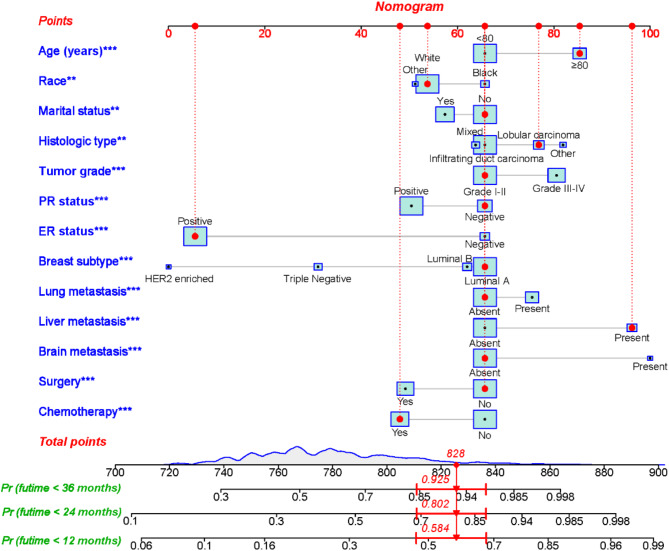
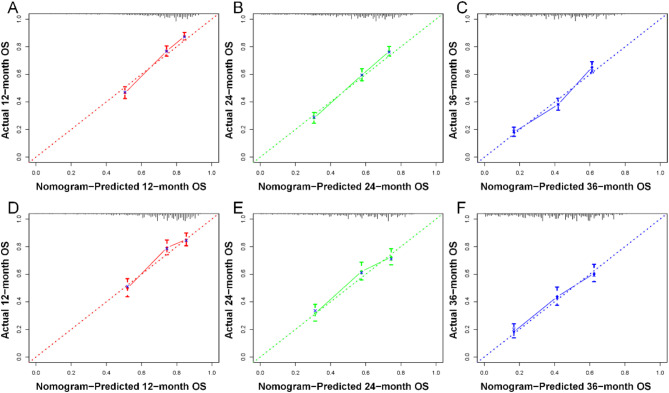
Breast cancer is currently the most common malignant tumor affecting women's health worldwide. The rise in breast cancer metastases among patients is attributed to the inherent variability in metastatic behavior. In breast cancer, bones are the primary location for distant metastases, significantly impacting the survival rates of elderly (≥ 65) patients. The use of surgery and chemotherapy in this population is controversial. This study seeks to create a tool for forecasting overall survival (OS) in older breast cancer patients with bone metastases and to determine the optimal candidates for surgery and chemotherapy. Elderly female breast cancer patients with bone metastases from the Surveillance, Epidemiology, and End Results (SEER) database were included in this study and categorized into a training cohort and a validation cohort using R software. To identify independent predictors of OS in this population, both univariate and multivariate Cox regression analyses were conducted. Subsequently, a prognostic nomogram was created to estimate OS at 12, 24, and 36 months. The nomogram's accuracy and practical value were assessed using a calibration curve, area under the curve (AUC), and decision curve analysis (DCA). At the same time, a mortality risk classification system based on the nomogram was created to divide the population into high and low mortality risk categories, and subgroups were analyzed to determine the optimal candidates for surgery and chemotherapy. This study encompassed 2257 elderly female breast cancer patients with bone metastases, divided into 1581 participants for the training cohort and 676 for the validation cohort. Both univariate and multivariate Cox regression analyses validated those variables such as age, race, marital status, histological type, tumor grade, ER status, PR status, breast subtype, distant metastases (lung, liver, and brain), and treatment methods (surgery and chemotherapy) independently predicted OS in elderly female breast cancer patients with bone metastases (p < 0.05). Utilizing these independent predictors, a prognostic nomogram was developed to estimate OS at 12, 24, and 36 months. The calibration curves indicated that the nomogram's predictions closely matched the observed outcomes. The nomogram's AUC for forecasting OS at 12, 24, and 36 months was 0.753, 0.748, and 0.745 in the training cohort, and 0.744, 0.723, and 0.723 in the validation cohort. Additionally, the nomogram's AUC surpassed that of any individual independent predictor. DCA showed that the nomogram could achieve more net clinical benefit over a broader range of threshold probabilities. The nomogram-based risk classification system effectively sorted patients into two categories: low risk (≤ 820) and high risk (> 820). Subgroup analysis indicated that individuals classified as low-risk experienced the greatest advantage from surgery and chemotherapy (p < 0.05), whereas the high-risk group did not exhibit a statistically significant difference (p > 0.05). Drawing from the clinicopathological characteristics of elderly female breast cancer patients with bone metastases, this study developed a novel prognostic nomogram to forecast OS at 12, 24, and 36 months, enabling precise survival predictions. In addition, this study also constructed a mortality risk classification system, which can effectively help clinicians screen out the optimal candidates to benefit from surgery and chemotherapy and rationalize the allocation of medical resources.
期刊介绍:
We publish original research from all areas of the natural sciences, psychology, medicine and engineering. You can learn more about what we publish by browsing our specific scientific subject areas below or explore Scientific Reports by browsing all articles and collections.
Scientific Reports has a 2-year impact factor: 4.380 (2021), and is the 6th most-cited journal in the world, with more than 540,000 citations in 2020 (Clarivate Analytics, 2021).
•Engineering
Engineering covers all aspects of engineering, technology, and applied science. It plays a crucial role in the development of technologies to address some of the world''s biggest challenges, helping to save lives and improve the way we live.
•Physical sciences
Physical sciences are those academic disciplines that aim to uncover the underlying laws of nature — often written in the language of mathematics. It is a collective term for areas of study including astronomy, chemistry, materials science and physics.
•Earth and environmental sciences
Earth and environmental sciences cover all aspects of Earth and planetary science and broadly encompass solid Earth processes, surface and atmospheric dynamics, Earth system history, climate and climate change, marine and freshwater systems, and ecology. It also considers the interactions between humans and these systems.
•Biological sciences
Biological sciences encompass all the divisions of natural sciences examining various aspects of vital processes. The concept includes anatomy, physiology, cell biology, biochemistry and biophysics, and covers all organisms from microorganisms, animals to plants.
•Health sciences
The health sciences study health, disease and healthcare. This field of study aims to develop knowledge, interventions and technology for use in healthcare to improve the treatment of patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


