Can nebulised heparin reduce acute lung injury in patients with SARS‑CoV‑2 requiring advanced respiratory support in Ireland: the CHARTER‑Ireland phase Ib/IIa, randomised, parallel-group, open-label study.
David Cosgrave, Bairbre McNicholas, Ciara Hanley, John Robert Sheehan, Padraig Calpin, Maeve Kernan, Darragh Murphy, Alberto Alvarez-Iglesias, John Ferguson, Camilla Giacomini, Christine Greene, Catriona Cody, Shane McGeary, Marion Murphy, Marianne Fitzgerald, Gerard Curley, Barry Dixon, Roger J Smith, Claire Masterson, Daniel O'Toole, Frank van Haren, John G Laffey
{"title":"Can nebulised heparin reduce acute lung injury in patients with SARS‑CoV‑2 requiring advanced respiratory support in Ireland: the CHARTER‑Ireland phase Ib/IIa, randomised, parallel-group, open-label study.","authors":"David Cosgrave, Bairbre McNicholas, Ciara Hanley, John Robert Sheehan, Padraig Calpin, Maeve Kernan, Darragh Murphy, Alberto Alvarez-Iglesias, John Ferguson, Camilla Giacomini, Christine Greene, Catriona Cody, Shane McGeary, Marion Murphy, Marianne Fitzgerald, Gerard Curley, Barry Dixon, Roger J Smith, Claire Masterson, Daniel O'Toole, Frank van Haren, John G Laffey","doi":"10.1186/s40635-025-00727-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Nebulised unfractionated heparin may attenuate COVID-19 ARDS by reducing pulmonary microvascular thrombosis, blocking SARS-CoV-2 entry into cells, and decreasing lung inflammation. COVID-19 patients with a raised D-dimer have areas of pulmonary hypoperfusion on CT perfusion scans of the lung and have increased mortality risk.</p><p><strong>Methods: </strong>This was a phase Ib/IIa open-label multi-centre, randomised controlled trial. The study was designed to evaluate whether nebulised unfractionated heparin decreased D-dimer concentrations, with safety as a co-primary outcome.</p><p><strong>Results: </strong>Forty patients were recruited, with 20 patients into each group. Mean age was 56.6 (SD 11.5) in the heparin group and 51.3 (SD 14.7) in the standard care group, while 60% of participants were male. There was no change in D-dimers from baseline to day 10 (heparin group mean change - 316.5, [SD 1840.3] and control group mean change - 321.7 [SD 3589.4]; p = 0.996). Fourteen patients suffered at least one serious adverse event, 9 patients the Heparin group and 5 in the control group. Eight patients had one or more bleeding events, 5 in the heparin group and 3 in the control group, but were no cases of pulmonary bleeding, of severe haemorrhage or of heparin-induced thrombocytopenia. Patients receiving heparin therapy had lower PaO<sub>2</sub>/FiO<sub>2</sub> ratios, increased oxygenation indices, and decreased ROX index profiles, up to day 10. The time to separation from respiratory support, and the time to ICU or hospital discharge was similar in both groups. There were 3 deaths in the Heparin group and 2 in the control group.</p><p><strong>Conclusions: </strong>Nebulised unfractionated heparin was safe and well tolerated, but did not reduce D-dimer concentrations, and worsened oxygenation indices in patients with COVID-19 ARDS.</p>","PeriodicalId":13750,"journal":{"name":"Intensive Care Medicine Experimental","volume":"13 1","pages":"15"},"PeriodicalIF":2.8000,"publicationDate":"2025-02-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11806160/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intensive Care Medicine Experimental","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40635-025-00727-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Nebulised unfractionated heparin may attenuate COVID-19 ARDS by reducing pulmonary microvascular thrombosis, blocking SARS-CoV-2 entry into cells, and decreasing lung inflammation. COVID-19 patients with a raised D-dimer have areas of pulmonary hypoperfusion on CT perfusion scans of the lung and have increased mortality risk.
Methods: This was a phase Ib/IIa open-label multi-centre, randomised controlled trial. The study was designed to evaluate whether nebulised unfractionated heparin decreased D-dimer concentrations, with safety as a co-primary outcome.
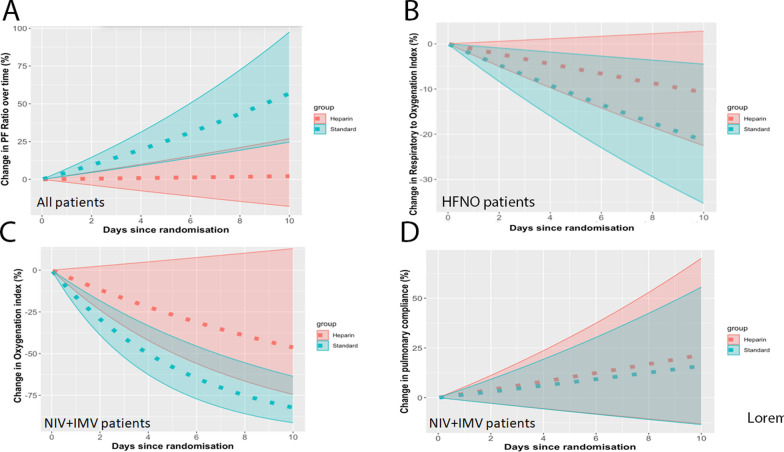
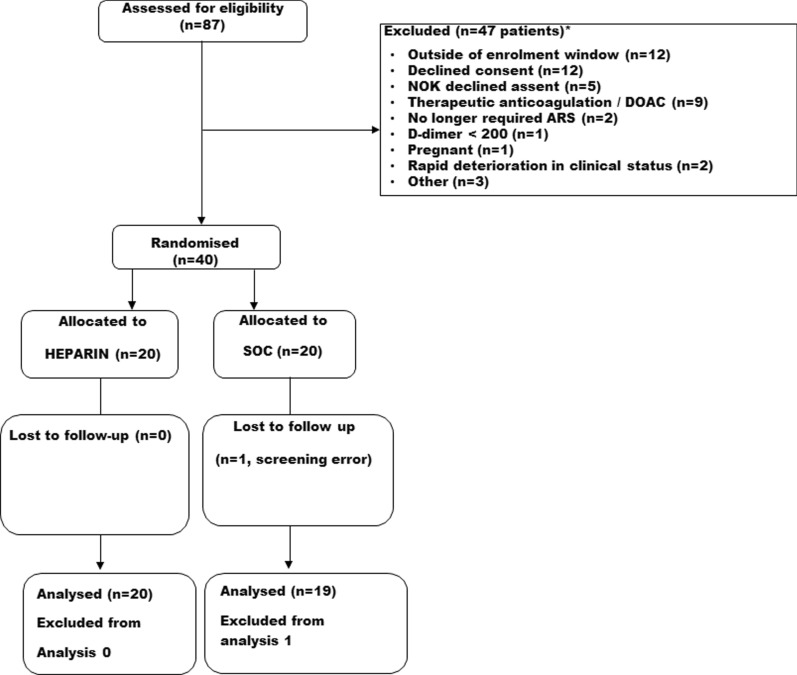
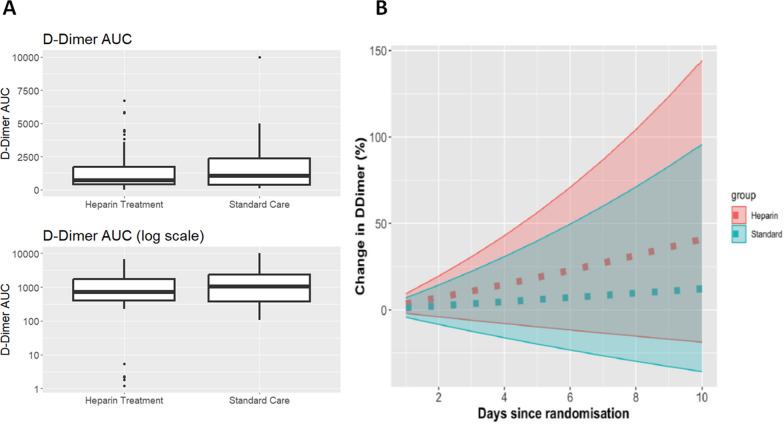
Results: Forty patients were recruited, with 20 patients into each group. Mean age was 56.6 (SD 11.5) in the heparin group and 51.3 (SD 14.7) in the standard care group, while 60% of participants were male. There was no change in D-dimers from baseline to day 10 (heparin group mean change - 316.5, [SD 1840.3] and control group mean change - 321.7 [SD 3589.4]; p = 0.996). Fourteen patients suffered at least one serious adverse event, 9 patients the Heparin group and 5 in the control group. Eight patients had one or more bleeding events, 5 in the heparin group and 3 in the control group, but were no cases of pulmonary bleeding, of severe haemorrhage or of heparin-induced thrombocytopenia. Patients receiving heparin therapy had lower PaO2/FiO2 ratios, increased oxygenation indices, and decreased ROX index profiles, up to day 10. The time to separation from respiratory support, and the time to ICU or hospital discharge was similar in both groups. There were 3 deaths in the Heparin group and 2 in the control group.
Conclusions: Nebulised unfractionated heparin was safe and well tolerated, but did not reduce D-dimer concentrations, and worsened oxygenation indices in patients with COVID-19 ARDS.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


