Aino Vesikansa, Juha Mehtälä, Sarah Smith, Anna Kirjavainen, Johanna Huupponen, Niina Säävuori, Katariina Pitkänen, Heikki Ukkonen
{"title":"Worsening Heart Failure and Medication Use in HFrEF: A Finnish Retrospective Registry Study and Patient Survey.","authors":"Aino Vesikansa, Juha Mehtälä, Sarah Smith, Anna Kirjavainen, Johanna Huupponen, Niina Säävuori, Katariina Pitkänen, Heikki Ukkonen","doi":"10.36628/ijhf.2024.0028","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Understanding worsening heart failure events (WHFEs) and clinical practices in the real world is essential in heart failure (HF) management. The primary objective of this single-center, retrospective, observational study, including a patient survey, was to characterize WHFEs and associated factors during the first year after the incident HF diagnosis in Finnish patients. Secondly, implementation and adherence to guideline-directed medical therapy (GDMT) and mortality during the whole follow-up were assessed.</p><p><strong>Methods: </strong>Incident HF patients (International Classification of Diseases, 10th Revision: I50) with reduced ejection fraction (HFrEF; <40%) were identified between 2013-2019 from the hospital data lake of Southwest Finland. Clinical characteristics, healthcare resource utilization, medication prescriptions and purchases, and deaths were collected from hospital records and national registers between 2011-2021. A survey was linked with register data for a subgroup of patients. Associations between explanatory factors, WHFEs, and mortality were studied using logistic and Cox regression models.</p><p><strong>Results: </strong>Among 570 HFrEF patients, 23% (n=133) experienced a WHFE within the first year after the incident diagnosis. During this 1-year period, 85% used angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, 90% beta-blockers, and 44% mineralocorticoid receptor antagonists, and >80% of patients were adherent to these medications. WHFEs were associated with higher risk of mortality (hazard ratio [HR], 1.82; 95% confidence interval [CI], 1.31-2.53; p<0.001), whereas adherence was associated with a lower risk of WHFEs (odds ratio, 0.31; 95% CI, 0.20-0.48; p<0.001) and mortality (HR, 0.66; 95% CI, 0.47-0.94; p=0.021) in multivariate models. Quality of life was lower in patients with (n=47) than without WHFEs (n=100).</p><p><strong>Conclusions: </strong>Improving adherence is crucial for mitigating adverse outcomes in HF.</p>","PeriodicalId":101410,"journal":{"name":"International journal of heart failure","volume":"7 1","pages":"6-18"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11791173/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International journal of heart failure","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36628/ijhf.2024.0028","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objectives: Understanding worsening heart failure events (WHFEs) and clinical practices in the real world is essential in heart failure (HF) management. The primary objective of this single-center, retrospective, observational study, including a patient survey, was to characterize WHFEs and associated factors during the first year after the incident HF diagnosis in Finnish patients. Secondly, implementation and adherence to guideline-directed medical therapy (GDMT) and mortality during the whole follow-up were assessed.
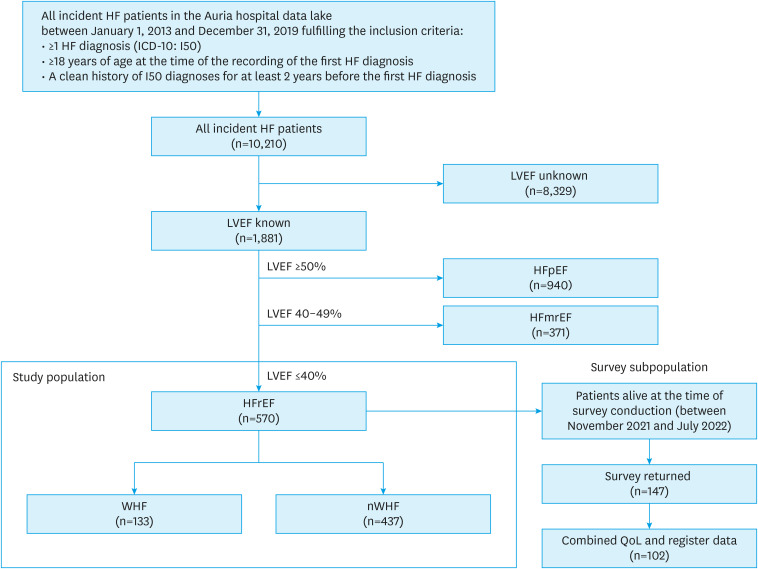
Methods: Incident HF patients (International Classification of Diseases, 10th Revision: I50) with reduced ejection fraction (HFrEF; <40%) were identified between 2013-2019 from the hospital data lake of Southwest Finland. Clinical characteristics, healthcare resource utilization, medication prescriptions and purchases, and deaths were collected from hospital records and national registers between 2011-2021. A survey was linked with register data for a subgroup of patients. Associations between explanatory factors, WHFEs, and mortality were studied using logistic and Cox regression models.
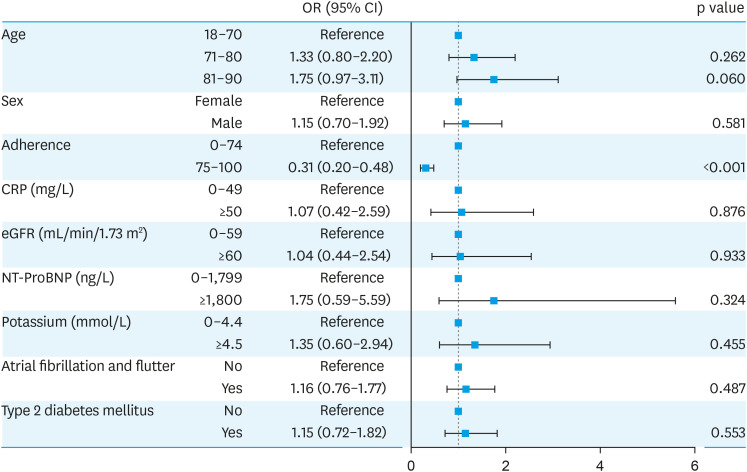
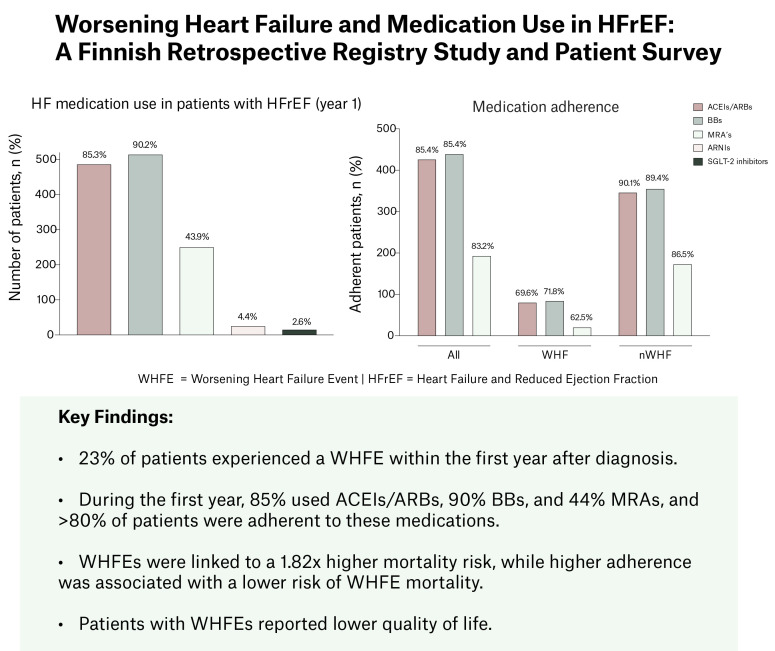
Results: Among 570 HFrEF patients, 23% (n=133) experienced a WHFE within the first year after the incident diagnosis. During this 1-year period, 85% used angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, 90% beta-blockers, and 44% mineralocorticoid receptor antagonists, and >80% of patients were adherent to these medications. WHFEs were associated with higher risk of mortality (hazard ratio [HR], 1.82; 95% confidence interval [CI], 1.31-2.53; p<0.001), whereas adherence was associated with a lower risk of WHFEs (odds ratio, 0.31; 95% CI, 0.20-0.48; p<0.001) and mortality (HR, 0.66; 95% CI, 0.47-0.94; p=0.021) in multivariate models. Quality of life was lower in patients with (n=47) than without WHFEs (n=100).
Conclusions: Improving adherence is crucial for mitigating adverse outcomes in HF.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


