Jeeyune Bahk, Harrindra Seepersaud, Matthew Alexander, Priscilla Loanzon, Adam Rothman, Susannah Kurtz, Joseph Mathew, James Salonia
{"title":"High-Fidelity Simulation Curriculum for Training Residents in Noninvasive Respiratory Support.","authors":"Jeeyune Bahk, Harrindra Seepersaud, Matthew Alexander, Priscilla Loanzon, Adam Rothman, Susannah Kurtz, Joseph Mathew, James Salonia","doi":"10.34197/ats-scholar.2023-0118OC","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> The coronavirus disease (COVID-19) pandemic highlighted the importance of physicians managing patients with noninvasive respiratory support (NIRS), including noninvasive ventilation (NIV) and high-flow nasal cannulas (HFNCs), emphasizing the need for thorough education on these modalities. <b>Objective:</b> To determine the effect of a novel simulation-based curriculum on improving the equipment familiarity and understanding of the physiology and application of NIRS among internal medicine residents. <b>Methods:</b> The curriculum consisted of a didactic session on the clinical application of NIRS, a case-based scenario on NIV using high-fidelity simulation, and a debrief session. Learners filled out surveys before and after the session to evaluate changes in objective knowledge of and subjective comfort with NIRS. <i>P</i> values were calculated using independent two-sample <i>t</i> tests. <b>Results:</b> Most residents (85.6%; <i>n</i> = 101) confirmed never having received a formal training in NIRS. At baseline, 34.7% (<i>n</i> = 41) and 24.6% (<i>n</i> = 29) felt \"comfortable\" or \"very comfortable,\" respectively, using NIRS, which improved to 91.5% (<i>n</i> = 108) and 89% (<i>n</i> = 105) after the session (<i>P</i> = 0.001). A statistically significant improvement in clinical knowledge was demonstrated after the session (<i>P</i> < 0.05), with residents correctly recognizing all three indications for bilevel positive airway pressure (BiPAP) (87.2% to 98.3%, 56% to 67.8%, and 21.2% to 55.1%), contraindications to BiPAP (81.4% to 90.7%), appropriate adjustment of BiPAP (30.5% to 73.7%), and HFNC settings (68.6% to 79.7%). Following the curriculum, postgraduate year (PGY)-1 (PGY-1)s' knowledge was increased beyond the baseline of the PGY-2/3s who trained in New York during the pandemic (mean score change 50.6% to 72.1% for PGY-1s, 61.5% to 75.7% for PGY-2/3s). Three-month retention surveys revealed consistent learner satisfaction and learner retention in all aspects. <b>Conclusion:</b> Our 1-hour high-fidelity simulation-based curriculum significantly enhanced medical residents' knowledge, skills, and confidence in using NIRS for acute respiratory failure, with particularly notable benefits for those in the early years of training. Such a simulation-based curriculum could potentially lead to better hospital resource allocation and improved patient outcomes.</p>","PeriodicalId":72330,"journal":{"name":"ATS scholar","volume":" ","pages":"52-64"},"PeriodicalIF":1.9000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11984655/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ATS scholar","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.34197/ats-scholar.2023-0118OC","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/7 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
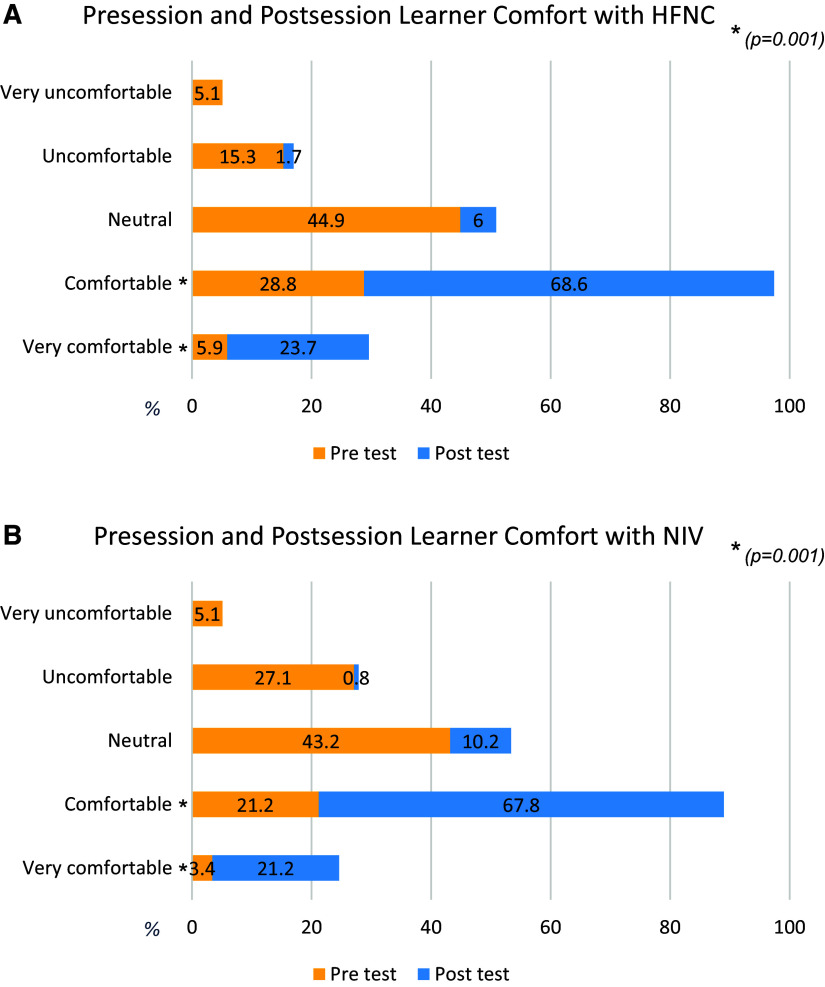
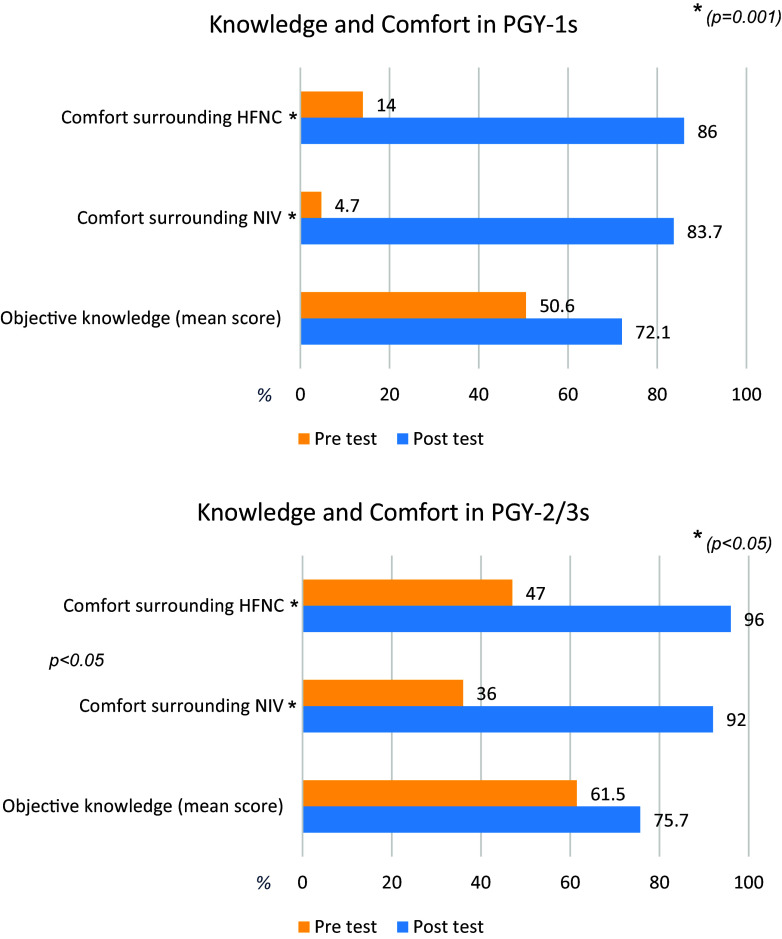
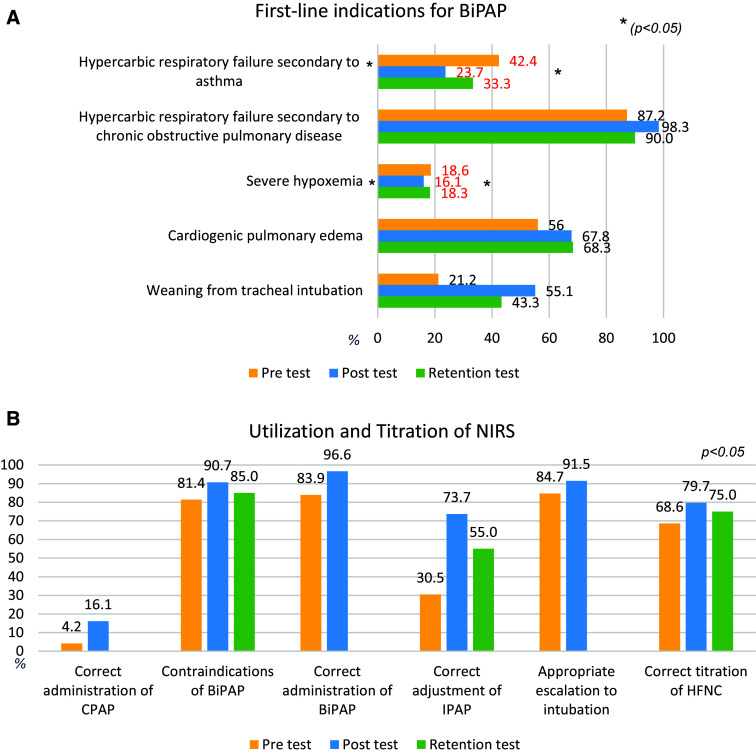
Background: The coronavirus disease (COVID-19) pandemic highlighted the importance of physicians managing patients with noninvasive respiratory support (NIRS), including noninvasive ventilation (NIV) and high-flow nasal cannulas (HFNCs), emphasizing the need for thorough education on these modalities. Objective: To determine the effect of a novel simulation-based curriculum on improving the equipment familiarity and understanding of the physiology and application of NIRS among internal medicine residents. Methods: The curriculum consisted of a didactic session on the clinical application of NIRS, a case-based scenario on NIV using high-fidelity simulation, and a debrief session. Learners filled out surveys before and after the session to evaluate changes in objective knowledge of and subjective comfort with NIRS. P values were calculated using independent two-sample t tests. Results: Most residents (85.6%; n = 101) confirmed never having received a formal training in NIRS. At baseline, 34.7% (n = 41) and 24.6% (n = 29) felt "comfortable" or "very comfortable," respectively, using NIRS, which improved to 91.5% (n = 108) and 89% (n = 105) after the session (P = 0.001). A statistically significant improvement in clinical knowledge was demonstrated after the session (P < 0.05), with residents correctly recognizing all three indications for bilevel positive airway pressure (BiPAP) (87.2% to 98.3%, 56% to 67.8%, and 21.2% to 55.1%), contraindications to BiPAP (81.4% to 90.7%), appropriate adjustment of BiPAP (30.5% to 73.7%), and HFNC settings (68.6% to 79.7%). Following the curriculum, postgraduate year (PGY)-1 (PGY-1)s' knowledge was increased beyond the baseline of the PGY-2/3s who trained in New York during the pandemic (mean score change 50.6% to 72.1% for PGY-1s, 61.5% to 75.7% for PGY-2/3s). Three-month retention surveys revealed consistent learner satisfaction and learner retention in all aspects. Conclusion: Our 1-hour high-fidelity simulation-based curriculum significantly enhanced medical residents' knowledge, skills, and confidence in using NIRS for acute respiratory failure, with particularly notable benefits for those in the early years of training. Such a simulation-based curriculum could potentially lead to better hospital resource allocation and improved patient outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


