Ara A Chrissian, Sevwandi De Silva, Erin Wiltchik, Brian Furukawa, Nico S Rizzo, Elliot Ho, Dafne Moretta, Gregory Cheek
{"title":"Impact of Pulmonary and Critical Care Fellow Participation during Advanced Diagnostic Bronchoscopy.","authors":"Ara A Chrissian, Sevwandi De Silva, Erin Wiltchik, Brian Furukawa, Nico S Rizzo, Elliot Ho, Dafne Moretta, Gregory Cheek","doi":"10.34197/ats-scholar.2024-0067OC","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Pulmonary and critical care medicine (PCCM) fellows frequently participate in advanced diagnostic bronchoscopy (ADB) procedures. <b>Objective:</b> To investigate the impact of PCCM fellow involvement during ADB on various procedural outcomes in a real-world setting. <b>Methods:</b> This was a retrospective observational cohort study analyzing prospectively collected registry data of consecutive ADB procedures performed between February 2018 and December 2021. Procedure duration, safety, breadth, and diagnostic performance of ADBs performed by PCCM fellows supervised by interventional pulmonologists (IPs) were compared with those completed solely by IP faculty. <b>Results:</b> Among 628 ADBs, fellows participated in 379 (60.3%). With unadjusted analysis, fellow-involved cases were a median 11.5 minutes longer for convex-probe endobronchial ultrasound bronchoscopy (95% confidence interval [CI], 6.0-14.0; <i>P</i> < 0.001) and 10.5 minutes longer for peripheral bronchoscopy (95% CI, 2.0-18.0; <i>P</i> = 0.016). Compared with ADBs performed by IP faculty alone, procedures with second-year (post-graduate year 5) fellows had the largest duration differences. These included convex-probe endobronchial ultrasound bronchoscopy (+14.5 min; 95% CI, 7.0-18.0 min; <i>P</i> < 0.001), cases not using rapid on-site evaluation (+14.0 min; 95% CI, 8.0-21.0 min; <i>P</i> < 0.001) and those performed with moderate sedation (+12.0 min; 95% CI, 7.0-18.0 min; <i>P</i> < 0.001). After multivariate adjustment, fellow-involved procedures overall were 7.2 minutes longer in duration (95% CI, 3.8-10.5; <i>P</i> < 0.001), and 8.8 minutes longer when performed by post-graduate year 5 fellows-an approximate 16% decrease in efficiency. Bronchoscopies performed with fellows were also more likely to experience complications (38.7% compared with 25.8% with faculty procedures; adjusted odds ratio [OR], 2.0; 95% CI, 1.3-3.0; <i>P</i> < 0.001) and be prematurely terminated (adjusted OR, 4.95; 95% CI, 1.44-17.02; <i>P</i> = 0.011). Diagnostic performance and occurrence of major complications were similar between fellow and no-fellow bronchoscopies. <b>Conclusion:</b> Participation of PCCM fellows during ADB increases procedure duration and the risk for minor complications compared with cases completed solely by IPs. Procedures performed with fellows on the steepest portion of the ADB learning curve are the least efficient. Fellowship directors and faculty bronchoscopists should acknowledge these potential impacts on ABD practice while optimizing the approach to bronchoscopy training.</p>","PeriodicalId":72330,"journal":{"name":"ATS scholar","volume":" ","pages":"36-51"},"PeriodicalIF":1.9000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11984652/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ATS scholar","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.34197/ats-scholar.2024-0067OC","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/30 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
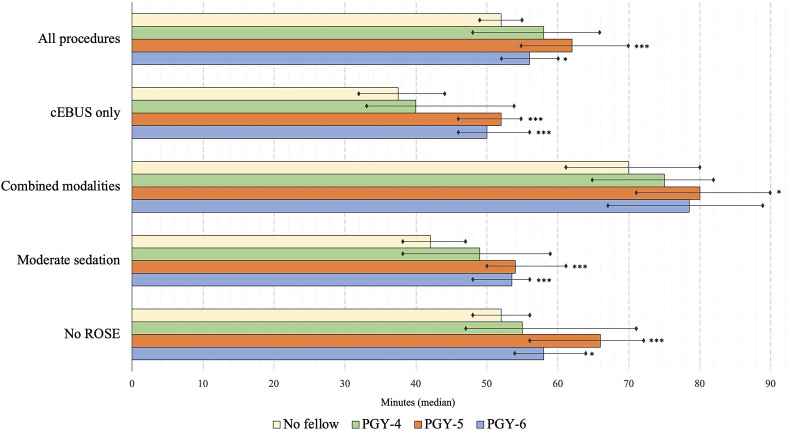
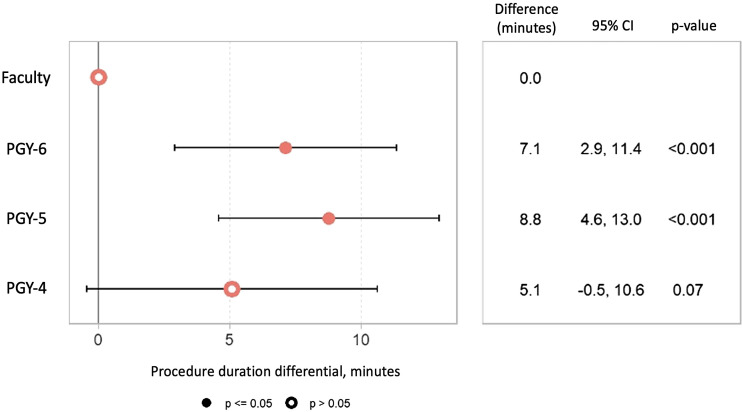
Background: Pulmonary and critical care medicine (PCCM) fellows frequently participate in advanced diagnostic bronchoscopy (ADB) procedures. Objective: To investigate the impact of PCCM fellow involvement during ADB on various procedural outcomes in a real-world setting. Methods: This was a retrospective observational cohort study analyzing prospectively collected registry data of consecutive ADB procedures performed between February 2018 and December 2021. Procedure duration, safety, breadth, and diagnostic performance of ADBs performed by PCCM fellows supervised by interventional pulmonologists (IPs) were compared with those completed solely by IP faculty. Results: Among 628 ADBs, fellows participated in 379 (60.3%). With unadjusted analysis, fellow-involved cases were a median 11.5 minutes longer for convex-probe endobronchial ultrasound bronchoscopy (95% confidence interval [CI], 6.0-14.0; P < 0.001) and 10.5 minutes longer for peripheral bronchoscopy (95% CI, 2.0-18.0; P = 0.016). Compared with ADBs performed by IP faculty alone, procedures with second-year (post-graduate year 5) fellows had the largest duration differences. These included convex-probe endobronchial ultrasound bronchoscopy (+14.5 min; 95% CI, 7.0-18.0 min; P < 0.001), cases not using rapid on-site evaluation (+14.0 min; 95% CI, 8.0-21.0 min; P < 0.001) and those performed with moderate sedation (+12.0 min; 95% CI, 7.0-18.0 min; P < 0.001). After multivariate adjustment, fellow-involved procedures overall were 7.2 minutes longer in duration (95% CI, 3.8-10.5; P < 0.001), and 8.8 minutes longer when performed by post-graduate year 5 fellows-an approximate 16% decrease in efficiency. Bronchoscopies performed with fellows were also more likely to experience complications (38.7% compared with 25.8% with faculty procedures; adjusted odds ratio [OR], 2.0; 95% CI, 1.3-3.0; P < 0.001) and be prematurely terminated (adjusted OR, 4.95; 95% CI, 1.44-17.02; P = 0.011). Diagnostic performance and occurrence of major complications were similar between fellow and no-fellow bronchoscopies. Conclusion: Participation of PCCM fellows during ADB increases procedure duration and the risk for minor complications compared with cases completed solely by IPs. Procedures performed with fellows on the steepest portion of the ADB learning curve are the least efficient. Fellowship directors and faculty bronchoscopists should acknowledge these potential impacts on ABD practice while optimizing the approach to bronchoscopy training.
背景:肺和重症医学(PCCM)研究员经常参加高级诊断支气管镜检查(ADB)程序。目的:探讨在现实世界中,PCCM同伴参与ADB对各种手术结果的影响。方法:这是一项回顾性观察性队列研究,分析了2018年2月至2021年12月期间连续行ADB手术的前瞻性收集注册数据。在介入肺科医师(IPs)的监督下,由PCCM研究员进行ADBs的手术时间、安全性、广度和诊断性能进行比较。结果:在628例adb中,研究员参与了379例(60.3%)。未经校正分析,同病病例接受凸探头支气管内超声支气管镜检查的平均时间延长11.5分钟(95%可信区间[CI], 6.0-14.0;p = 0.016)。与仅由知识产权学院教员执行的adb相比,由二年级(研究生五年级)教员执行的程序持续时间差异最大。包括凸探头支气管内超声支气管镜检查(+14.5 min;95% CI, 7.0-18.0 min;p p p p p p = 0.011)。同组和非同组支气管镜检查的诊断表现和主要并发症的发生相似。结论:与完全由IPs完成的病例相比,PCCM研究员参与ADB增加了手术时间和轻微并发症的风险。在亚行学习曲线最陡峭的部分,由研究员执行的程序效率最低。奖学金主任和教师支气管镜医师在优化支气管镜培训方法时应认识到这些对ABD实践的潜在影响。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


