{"title":"[A case of sepsis complicated by multiple organ dysfunction syndrome with CT appearance of pseudo-subarachnoid hem-orrhage].","authors":"Yan Qi","doi":"10.3724/zdxbyxb-2024-0022","DOIUrl":null,"url":null,"abstract":"<p><p>A 39-year-old male patient was admitted to hospital with abdominal distension, unconsciousness, and anuria. Head computed tomography (CT) showed subarachnoid hemorrhage and diffuse cerebral edema. The high-density area of contrast accumulation region in the high-density CT plaque was 38 HU, and the preliminary diagnosis was SAH, incomplete intestinal obstruction, and sepsis caused by acute cerebrovascular disease. After admission, the patient displayed upturned eyes, limb convulsions, serum procalcitonin level exceeding 100 ng/mL, low blood pressure and septic shock. Imipenem was given for intensive anti-infection therapy. After treatment, procalcitonin levels showed a slow decline, renal function, and intra-abdominal pressure returned to normal, urine volume gradually increased, but platelets still showed a downward trend. Lumbar puncture showed colorless and clear cerebrospinal fluid, and the biochemical and routine results of cerebrospinal fluid were normal. SAH and intracranial infection were excluded, and it was considered that the head CT showed pseudo-subarachnoid hemorrhage. On the 3rd day of admission, laparoscopic exploratory laparotomy+appendectomy+abdominal drainage under general anesthesia were performed. During surgery, purulent gangrene in the appendix was found, with pus adhering to the surface of the intestines and a large amount of pus present in the abdominal cavity. Rhabdomyolysis syndrome developed after surgery. After continuous renal replacement therapy, the indicators gradually returned to normal. The patient was conscious, and the head CT results were normal. The patient was discharged from the hospital on the 19th day after surgery, and no special discomfort and abdominal pain and distension occurred during the 3-month follow-up.</p>","PeriodicalId":24007,"journal":{"name":"Zhejiang da xue xue bao. Yi xue ban = Journal of Zhejiang University. Medical sciences","volume":" ","pages":"115-119"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11886950/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Zhejiang da xue xue bao. Yi xue ban = Journal of Zhejiang University. Medical sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3724/zdxbyxb-2024-0022","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
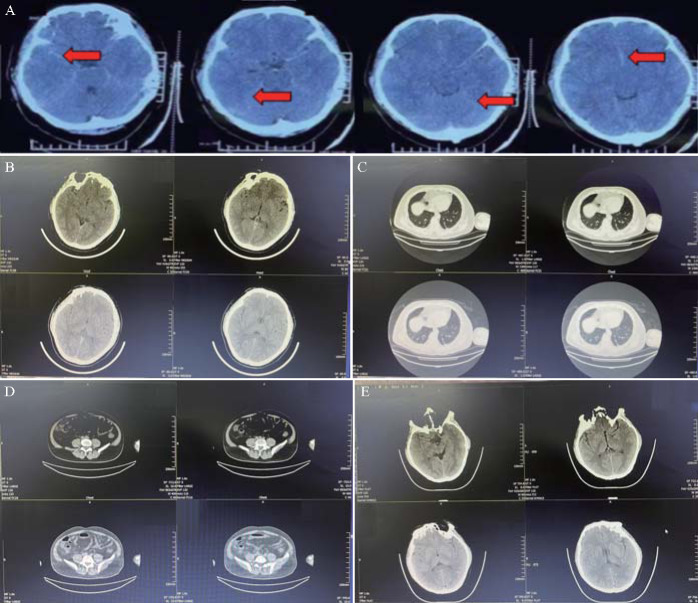
A 39-year-old male patient was admitted to hospital with abdominal distension, unconsciousness, and anuria. Head computed tomography (CT) showed subarachnoid hemorrhage and diffuse cerebral edema. The high-density area of contrast accumulation region in the high-density CT plaque was 38 HU, and the preliminary diagnosis was SAH, incomplete intestinal obstruction, and sepsis caused by acute cerebrovascular disease. After admission, the patient displayed upturned eyes, limb convulsions, serum procalcitonin level exceeding 100 ng/mL, low blood pressure and septic shock. Imipenem was given for intensive anti-infection therapy. After treatment, procalcitonin levels showed a slow decline, renal function, and intra-abdominal pressure returned to normal, urine volume gradually increased, but platelets still showed a downward trend. Lumbar puncture showed colorless and clear cerebrospinal fluid, and the biochemical and routine results of cerebrospinal fluid were normal. SAH and intracranial infection were excluded, and it was considered that the head CT showed pseudo-subarachnoid hemorrhage. On the 3rd day of admission, laparoscopic exploratory laparotomy+appendectomy+abdominal drainage under general anesthesia were performed. During surgery, purulent gangrene in the appendix was found, with pus adhering to the surface of the intestines and a large amount of pus present in the abdominal cavity. Rhabdomyolysis syndrome developed after surgery. After continuous renal replacement therapy, the indicators gradually returned to normal. The patient was conscious, and the head CT results were normal. The patient was discharged from the hospital on the 19th day after surgery, and no special discomfort and abdominal pain and distension occurred during the 3-month follow-up.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


