{"title":"Multicenter Prospective First-Line Helicobacter Pylori Eradication for Localized Gastric “Pure” Diffuse Large B-Cell Lymphoma","authors":"Li-Tzong Chen, Kun-Huei Yeh, Chung-Wu Lin, Tsang-En Wang, Ming-Chung Wang, Chin-Fu Hsiao, Chieh-Chang Chen, Jyh-Ming Liou, Hsiu-Po Wang, Ming-Feng Wei, Hsiao-Wei Lee, Chia-Tung Shun, Tsang-Wu Liu, Hwei-Fang Tien, Ming-Shiang Wu, Sung-Hsin Kuo, Ann-Lii Cheng","doi":"10.1002/ajh.27624","DOIUrl":null,"url":null,"abstract":"<p>Our exploratory study evaluated the efficacy of first-line <i>Helicobacter pylori</i> eradication (HPE) therapy on early-stage (stage IE/IIE1) <i>Helicobacter pylori</i> (HP)-positive gastric diffuse large B-cell lymphomas (DLBCLs) without histological evidence of mucosa-associated lymphoid tissue (MALT) (“pure” DLBCLs). The study showed that 11 of 16 (68.8%) patients achieved complete remission (CR) after successful HPE and remained lymphoma-free after a median follow-up of 7.7 years [<span>1</span>]. Another study by Tari et al. demonstrated that 4 of 15 (26.7%) patients with gastric “pure” DLBCLs who received first-line antibiotic treatment achieved CR and remained lymphoma-free after a median follow-up of 7–100 months [<span>2</span>]. Additionally, Ferrieri et al. studied 16 patients with gastric DLBCLs, of whom, 11 had “pure” DLBCLs and five had DLBCLs with histological evidence of MALT (DLBCL[MALT]), who were administered HPE (including clarithromycin, tinidazole or metronidazole, and omeprazole) [<span>3</span>]. Of these, eight patients achieved CR and three achieved partial remission (PR), with an overall response rate (ORR) of 68.8% after HPE [<span>3</span>]. Cumulatively, these findings indicate that certain patients with gastric “pure” DLBCLs are responsive to first-line antibiotic therapy and might have a better quality of life because they are not exposed to the conventional immunochemotherapy-related adverse effects. However, prospective studies evaluating patients whose tumors are not limited to the stomach but extend to the perigastric lymph node area are warranted.</p>\n<p>Considering that “pure” DLBCLs of the stomach grow rapidly when the tumors do not respond to first-line HPE, identifying molecular markers that can predict HP independence (the lack of CR of tumors after completing HPE) is necessary. Our previous study showed that in in vitro DLBCL cell lines, B cell activating factor (BAFF) triggered the activation of NF-κB. Furthermore, it caused nuclear translocation of BCL10 by inducing AKT phosphorylation and disrupting the interaction of BCL10 with MALT1 and subsequent complex formation of BCL10 and BCL3 (nuclei translation-related genes) [<span>4</span>]. Furthermore, in tumor samples from patients with gastric DLBCL(MALT)s who received first-line HPE, BAFF overexpression was significantly associated with the nuclear translocation of BCL10 or NF-κB (p65), and the aforementioned molecules (including BAFF, nuclear BCL10, and nuclear NF-κB (p65)) were significantly correlated with HP independence of the tumor [<span>4</span>]. In contrast to HP-independent biomarkers, we detected HP-encoded protein cytotoxin-associated gene A (CagA) in tumor samples of patients with gastric MALT lymphomas and DLBCL(MALT)s [<span>5, 6</span>]. The expression of CagA was more frequent in HP-dependent tumors than in HP-independent tumors of gastric lymphomas [<span>5, 6</span>].</p>\n<p>In March 2015, the National Taiwan University and the National Health Research Institutes of Taiwan initiated a prospective phase II, multicenter trial named the Taiwan Cooperative Oncology Group (TCOG) 2214 trial, registered at ClinicalTrials.gov (NCT02388581). This trial assessed the treatment efficacy of first-line HPE treatment and the predictivity of the HP-dependent marker—CagA and of HP-independent markers—BAFF and nuclear expression of BCL10 or NF-κB (p65)—in early-stage (stages IE and IIE1) HP-positive gastric “pure” DLBCLs. Patients who had histologically confirmed stage IE and IIE1 primary gastric “pure” DLBCLs and had no prior chemotherapy or radiotherapy for his/her gastric “pure” DLBCLs were enrolled. Detailed information on histological diagnosis and criteria of “pure” DLBCL, staging work-up, diagnosis of HP infection, HPE regimen, clinical follow-up, and the histological scoring system of the Groupe d'Etude des Lymphomes de l'Adult (GELA) [<span>7</span>] for assessing lymphoma responses toward HPE are provided in Supplementary Methods. The experimental methods for immunohistochemical detection of CagA, BCL10, NF-κB (p65), BAFF, CD10, BCL6, and MUM-1, interphase fluorescence in situ hybridization for assessing t(11;18)(q21;q21), primary endpoints, secondary endpoints, and statistical analyses are provided in the Supplementary Methods [<span>6, 8</span>]. All patients provided written informed consent for follow-ups and agreed to provide pathological samples for translational studies. All experimental protocols were approved by the Institutional Review Board (IRB) of the Research Ethical Committee of the National Taiwan University Hospital (NTUH) (NTUH IRB numbers: 201411005MINA).</p>\n<p>Between March 2015 and September 2020, a total of 18 patients with stage IE/IIE1 HP-positive gastric “pure” DLBCLs who met the eligibility criteria were recruited. The cohort comprised eight men and 10 women (median age, 66 years; range, 23–89 years). Among them, 15 patients were diagnosed with HP infection based on a positive histological examination or rapid urease test, and three had a positive <sup>13</sup>C urea breath test. The most common symptom was epigastric discomfort. Before participating in the clinical trial, two patients had undergone 1 week of HPE regimen for treating ulcers and gastric discomforts. These two patients were diagnosed with HP infection (one based on histology examination and the other based on <sup>13</sup>C urea breath test) before starting our HPE regimen protocol. The clinicopathological features of the enrolled 18 patients are outlined in Table S1. Initially, HP infection was successfully eradicated in two of five (40%) patients after they underwent first-line sequential HPE regimen (Figure S1). After shifting to quadruple antibiotic therapy (Figure 1A), 12 of 13 (92.3%), patients achieved successful HPE. Four patients with “pure” DLBCLs exhibited persistent HP infection after the first-line antibiotic therapy and were subsequently, immediately treated with systemic immunochemotherapy for avoiding progressive disease (PD) (Figure 1A). Grade 1 adverse effects such as nausea, diarrhea, and constipation were reported in patients administered with HPE regimens. No adverse effects of grades 2, 3, or 4 were reported.</p>\n<figure><picture>\n<source media=\"(min-width: 1650px)\" srcset=\"/cms/asset/784d133e-3e3e-4a40-a86f-32a8789f3910/ajh27624-fig-0001-m.jpg\"/><img alt=\"Details are in the caption following the image\" data-lg-src=\"/cms/asset/784d133e-3e3e-4a40-a86f-32a8789f3910/ajh27624-fig-0001-m.jpg\" loading=\"lazy\" src=\"/cms/asset/5d458889-74b3-499d-abe4-83ae11164b7b/ajh27624-fig-0001-m.png\" title=\"Details are in the caption following the image\"/></picture><figcaption>\n<div><strong>FIGURE 1<span style=\"font-weight:normal\"></span></strong><div>Open in figure viewer<i aria-hidden=\"true\"></i><span>PowerPoint</span></div>\n</div>\n<div>The schema, clinical courses, and clinical outcomes of first-line <i>Helicobacter pylori</i> eradication therapy (HPE) for stage IE/IIE1 gastric “pure” DLBCL. (A) The schema for bismuth quadruple HPE regimen, biological markers, follow-up, and salvage treatment if no response to HPE. (B) Time to CR in seven patients with gastric “pure” DLBCLs, as calculated from the completion of antibiotic treatment to the first evidence of CR through Kaplan–Meier analysis. (C) Duration of CR, time to chemotherapy for patients without CR, relapse status, survival, and ongoing status of all patients. *: The presence of HP infection is defined as a positive result, based on biopsy, histology, rapid urease test, <sup>13</sup>C urea breath test, serology, or culture. **: The presence of t(11;18)(q21;q21) was assessed by the interphase fluorescence in situ hybridization (FISH) method using a commercially available probe (<i>BIRC3/MALT1</i> dual-color, dual-fusion translocation probe; Vysis LSI/Abbott). The expressions of BCL10, NF-κB (p65), BAFF, and CagA were assessed by immunohistochemistry (IHC). Abbreviation: CR, complete remission; PR, partial remission; SD, stable disease; PD, progressive disease.</div>\n</figcaption>\n</figure>\n<p>Of the 18 patients administered with first-line HPE, seven (38.9%) achieved CR and three (16.7%) achieved PR, with an ORR of 55.6% (95% confidence interval [CI], 30.1%–80.9%) determined based on the criteria of the GELA scoring system. Figure 2 illustrates alterations in the endoscopic findings and histological characteristics in a representative case of CR. In the 14 patients who achieved successful HP eradication, first-line HPE resulted in an ORR of 71.4% (CR = 7 [50.0%], PR = 3 [21.4%]; 95% CI, 44.3%–98.5%). The median time to CR after completion of HPE for all patients (<i>n</i> = 7) who achieved CR was 4.00 months (95% CI, 0.49–7.51 months; range 1–7 months) (Figure 1B). All seven patients who achieved CR after HPE were alive and DLBCL-free, and the median CR duration was 69.2 months (95% CI, 34.8–103.6 months; range, 38.4–81.4 months) (Figure 1C). Figure 3A–E present alterations in endoscopic examination findings and 18F-FDG <i>PET/CT</i> image findings for representative patients with CR, with long-term CR after completion of HPE.</p>\n<figure><picture>\n<source media=\"(min-width: 1650px)\" srcset=\"/cms/asset/1d18558c-170e-49b5-9aee-2e45d6acb8be/ajh27624-fig-0002-m.jpg\"/><img alt=\"Details are in the caption following the image\" data-lg-src=\"/cms/asset/1d18558c-170e-49b5-9aee-2e45d6acb8be/ajh27624-fig-0002-m.jpg\" loading=\"lazy\" src=\"/cms/asset/143d6a94-c037-4427-b7b3-61cc262cbaf5/ajh27624-fig-0002-m.png\" title=\"Details are in the caption following the image\"/></picture><figcaption>\n<div><strong>FIGURE 2<span style=\"font-weight:normal\"></span></strong><div>Open in figure viewer<i aria-hidden=\"true\"></i><span>PowerPoint</span></div>\n</div>\n<div>Endoscopic and histopathological manifestations in a patient with gastric “pure” DLBCLs who completely responded to first-line <i>Helicobacter pylori</i> eradication therapy (HPE). (A) Before HPE, multiple larger ulcerative lesions with elevated and swelling borders up to 4 cm in diameter are found at the antrum, angle, and lower body of the stomach (Endoscopic ultrasonography [EUS] showing tumor with involvement of muscularis propria layers [maximum thickness: 14.1 mm], left bottom inset). One month after completing HPE, three protruding ulcerative tumors are found at the antrum and lower body of stomach, and partial remission (PR) is achieved (EUS, maximum thickness: 12.6 mm, left bottom inset). Four months after completing HPE, two protruding tumors with improved ulceration and continued PR are found at the antrum of stomach (EUS, maximum thickness: 8.5 mm, right upper inset). Seven months after completing HPE, complete remission (CR) of ulcerative mass with hyperemic patches is observed at the antrum of the stomach (EUS, right upper inset). (B) A CT scan performed before HPE shows gastric wall thickness at the antrum and lower body of the stomach (axial and coronal view, white arrow). Four months after completing HPE, PR of gastric wall thickness is observed (coronal view, white arrow), and CR is observed at 7 months after completion of HPE (coronal view, white arrow). (C) Before HPE, hematoxylin and eosin stain (H&E) staining (upper panel 100×; lower panel 400×): Biopsy of ulcerative mass of antrum shows diffuse large lymphoid cells (enlarged nuclei and vesicular chromatin pattern) infiltrating the lamina propria (right upper inset, large cells are positive for CD20). Four months after completing HPE, H&E staining (upper panel 100×; lower panel 400×) shows immunoblast-like large lymphoid cells infiltrating the lamina propria. Seven months after completing HPE, H&E staining (upper panel 100×; lower panel 400×) shows chronic gastritis with lymphoplasma cells infiltration in the mucosal glands and lamina propria.</div>\n</figcaption>\n</figure>\n<figure><picture>\n<source media=\"(min-width: 1650px)\" srcset=\"/cms/asset/493bb17a-06ce-41ad-b407-9e5664a37d3e/ajh27624-fig-0003-m.jpg\"/><img alt=\"Details are in the caption following the image\" data-lg-src=\"/cms/asset/493bb17a-06ce-41ad-b407-9e5664a37d3e/ajh27624-fig-0003-m.jpg\" loading=\"lazy\" src=\"/cms/asset/99245874-7c47-4e8c-966a-ed76b54645c4/ajh27624-fig-0003-m.png\" title=\"Details are in the caption following the image\"/></picture><figcaption>\n<div><strong>FIGURE 3<span style=\"font-weight:normal\"></span></strong><div>Open in figure viewer<i aria-hidden=\"true\"></i><span>PowerPoint</span></div>\n</div>\n<div>Endoscopic examination and 18F-FDG <i>PET/CT</i> examination of a patient with long-term CR after first-line HPE, and survival curve of all patients with gastric “pure” DLBCLs who received first-line HPE. (A) Endoscopy shows enlarged gastric folds with multiple nodularity and ulceration (the largest one was found 2 cm in size in the middle body) at the greater curvature of gastric lower body, extending to the greater curvature of the gastric upper body in an 73-year-old woman before HPE (histopathology revealed “pure” DLBCL without histological evidence of mucosa-associated lymphoid tissue). (B) A <i>PET/CT</i> reveals intense hot areas (white arrow) along the greater curvature of the gastric wall (standard uptake value max = 34.19) (axial, coronal, and sagittal views). (C) The patient achieved CR 7 months after completing HPE, as documented by endoscopic examination and histologic manifestations. (D) At 17 months after completion of HPE, endoscopy shows CR with gastritis and scattered scars in the middle body of the stomach <i>in the same case presented in (A)</i>. (E) At 24 months after completing HPE, PET/CT reveals still CR with completely resolved prior gastric lymphoma in the same case <i>presented in (A)</i> (Deauville score = 2). (F) The event-free survival curve and the overall survival for all cases. Abbreviations: PET, positron emission tomography; CT, computed tomography; CR, complete remission; HPE, <i>Helicobacter pylori</i> eradication therapy; EFS, event-free survival; OS, overall survival.</div>\n</figcaption>\n</figure>\n<p>In the current study, among patients without CR (<i>n</i> = 11), most were older (age range 58–89 years, except for one patient who was 23 years old) and had age-related comorbidities. Considering their elderly status and comorbidities and that these patients may be intolerant to conventional chemotherapy (CHOP, cyclophosphamide, doxorubicin, vincristine, and prednisolone)-associated adverse effects, patients without CR were treated with a rituximab (R)-based regimen (most R-COP [cyclophosphamide, vincristine, and prednisolone], except for one patient who was 89 years old and was treated with rituximab plus prednisolone [RP], and one patient [23 years] received R-CHOP). The information on age and age-related comorbidities of patients with gastric “pure” DLBCL who received a rituximab (R)-based regimen after failing to completely respond to frontline HPE regimens is listed in Table S2. Three patients achieved PR at the first follow-up conducted 1 month after completing HPE and were administered subsequent immunochemotherapy consisting of R-COP (<i>n</i> = 2) or RP (<i>n</i> = 1) at 7, 9, and 10 months for the first, second, and third patient, respectively, because of progressive symptoms and disease during follow-up of endoscopic or abdominal CT scan examinations (Figure 1A,C). Notably, these three patients achieved CR after being administered immunochemotherapy. Of the eight patients who did not respond to HPE (stable disease [SD], <i>n</i> = 5; PD, <i>n</i> = 3), seven were treated with R-COP and one with R-CHOP; all of them subsequently achieved CR (Figure 1A,C). After a median follow-up of 61.1 months (95% CI; 46.3–75.9 months; range 7.0–103.1 months), only one patient died from pneumonia unrelated to lymphoma. Another patient who exhibited initial PD after HPE and achieved CR after being administered R-COP, developed local relapse of gastric DLBCL after 2 years and again achieved CR after being administered R-CHOP (Figure 1C). The 5-year event-free survival rate for all patients was 88.9% (95% CI, 74.4%–100%), and the 5-year overall survival rate for all patients was 94.4% (95% CI, 83.8%–100%) (Figure 3F).</p>\n<p>The main clinicopathological features of the seven patients who achieved CR and the 11 who did not, and their responses to HPE are summarized in Table 1. No statistically significant differences were observed for age, sex, endoscopic appearance, stage, or tumor location between patients with CR and non-CR tumors. Tumor size < 5 cm (endoscopic extended maximal size) (<i>p</i> = 0.05) and tumor invasion less than the muscularis propria (<i>p</i> = 0.063) were associated with CR status (Table 1). Nuclear BCL10 expression (<i>p</i> = 0.004), nuclear NF-κB (p65) expression (<i>p</i> = 0.004), and BAFF expression (<i>p</i> = 0.0498) were significantly associated with non-CR status, whereas GCB subtype was not associated with CR status (according to the Hans algorithm) (Table 1, Figures S2 and S3A,B). However, we found no significant differences of CagA expression, nuclear BCL10 expression, nuclear NF-κB (p65) expression, and BAFF expression in tumor cells between patients with CR and those with PR (Table S3). When we classified our patients as those with responsive tumors (CR and PR, <i>n</i> = 10) and those with non-responsive tumors (SD and PD, <i>n</i> = 8), we found that sex (<i>p</i> = 0.025), tumor size < 5 cm (<i>p</i> = 0.015), presence of CagA expression (<i>p</i> = 0.023), absence of nuclear expression of BCL10 (<i>p</i> = 0.003) and NF-κB (p65) (<i>p</i> = 0.003), and BAFF expression (<i>p</i> = 0.015) were significantly associated with the tumor response to HPE (Table S4).</p>\n<div>\n<header><span>TABLE 1. </span>Differential clinicopathologic features and molecular markers between patients with CR and those without CR tumors.</header>\n<div tabindex=\"0\">\n<table>\n<thead>\n<tr>\n<th>Characteristics</th>\n<th>Total (<i>N</i> = 18)</th>\n<th>CR-tumors (<i>N</i> = 7)</th>\n<th>Non-CR tumors (<i>N</i> = 11)</th>\n<th>\n<i>p</i>\n</th>\n</tr>\n</thead>\n<tbody>\n<tr>\n<td>Age</td>\n<td></td>\n<td></td>\n<td></td>\n<td>0.447</td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Median (range)</td>\n<td>66.5 (23–89)</td>\n<td>67.0 (36–73)</td>\n<td>66.0 (23–89)</td>\n<td></td>\n</tr>\n<tr>\n<td>Sex</td>\n<td></td>\n<td></td>\n<td></td>\n<td>0.145</td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Women</td>\n<td>10 (55.6%)</td>\n<td>2 (28.6%)</td>\n<td>8 (72.7%)</td>\n<td></td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Men</td>\n<td>8 (44.4%)</td>\n<td>5 (71.4%)</td>\n<td>3 (27.3%)</td>\n<td></td>\n</tr>\n<tr>\n<td>Endoscopic appearance</td>\n<td></td>\n<td></td>\n<td></td>\n<td>0.605</td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Ulcerative lesion</td>\n<td>14 (77.8%)</td>\n<td>5 (71.4%)</td>\n<td>9 (81.8%)</td>\n<td></td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Non-ulcerative lesion</td>\n<td>4 (22.2%)</td>\n<td>2 (28.1%)</td>\n<td>2 (18.2%)</td>\n<td></td>\n</tr>\n<tr>\n<td>Location</td>\n<td></td>\n<td></td>\n<td></td>\n<td>0.620</td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Proximal<sup>&</sup></td>\n<td>6 (33.7%)</td>\n<td>1 (14.3%)</td>\n<td>5 (45.5%)</td>\n<td></td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Distal<sup>#</sup></td>\n<td>12 (67.3%)</td>\n<td>6 (85.7%)</td>\n<td>6 (54.5%)</td>\n<td></td>\n</tr>\n<tr>\n<td>Tumor size</td>\n<td></td>\n<td></td>\n<td></td>\n<td>0.050</td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">≥ 5 cm</td>\n<td>9 (50.0%)</td>\n<td>1 (14.3%)</td>\n<td>8 (72.7%)</td>\n<td></td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">< 5 cm</td>\n<td>9 (50.0%)</td>\n<td>6 (85.7%)</td>\n<td>3 (27.3%)</td>\n<td></td>\n</tr>\n<tr>\n<td>Stage</td>\n<td></td>\n<td></td>\n<td></td>\n<td>0.605</td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">IE1</td>\n<td>14 (77.8%)</td>\n<td>5 (71.4%)</td>\n<td>9 (81.8%)</td>\n<td></td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">IIE1</td>\n<td>4 (22.2%)</td>\n<td>2 (28.6%)</td>\n<td>2 (18.2%)</td>\n<td></td>\n</tr>\n<tr>\n<td>Tumor invasiveness*</td>\n<td></td>\n<td></td>\n<td></td>\n<td>0.063</td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Mucosa/submucosa</td>\n<td>3 (18.8%)</td>\n<td>3 (42.9%)</td>\n<td>0 (0.0%)</td>\n<td></td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Muscularis/serosa/IIE1</td>\n<td>13 (81.2%)</td>\n<td>4 (57.1%)</td>\n<td>9 (100%)</td>\n<td></td>\n</tr>\n<tr>\n<td>CagA expression</td>\n<td></td>\n<td></td>\n<td></td>\n<td>0.119</td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Positive</td>\n<td>14 (77.8%)</td>\n<td>7 (100%)</td>\n<td>7 (63.6%)</td>\n<td></td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Negative</td>\n<td>4 (22.2%)</td>\n<td>0 (0.0%)</td>\n<td>4 (36.4%)</td>\n<td></td>\n</tr>\n<tr>\n<td>Nuclear BCL10 expression</td>\n<td></td>\n<td></td>\n<td></td>\n<td>0.004</td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Positive</td>\n<td>8 (44.4%)</td>\n<td>0 (0.0%)</td>\n<td>8 (72.7%)</td>\n<td></td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Negative</td>\n<td>10 (55.6%)</td>\n<td>7 (100%)</td>\n<td>3 (27.3%)</td>\n<td></td>\n</tr>\n<tr>\n<td>Nuclear NF-κB (p65) expression</td>\n<td></td>\n<td></td>\n<td></td>\n<td>0.004</td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Positive</td>\n<td>8 (44.4%)</td>\n<td>0 (0.0%)</td>\n<td>8 (72.7%)</td>\n<td></td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Negative</td>\n<td>10 (55.6%)</td>\n<td>7 (100%)</td>\n<td>3 (27.3%)</td>\n<td></td>\n</tr>\n<tr>\n<td>BAFF overexpression</td>\n<td></td>\n<td></td>\n<td></td>\n<td>0.0498</td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Positive</td>\n<td>9 (50%)</td>\n<td>1 (14.3%)</td>\n<td>8 (72.7%)</td>\n<td></td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Negative</td>\n<td>9 (50%)</td>\n<td>6 (85.7%)</td>\n<td>3 (27.3%)</td>\n<td></td>\n</tr>\n<tr>\n<td>GCB/non-GCB</td>\n<td></td>\n<td></td>\n<td></td>\n<td>0.367</td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">GCB</td>\n<td>10 (55.6%)</td>\n<td>5 (71.4%)</td>\n<td>5 (45.5%)</td>\n<td></td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Non-GCB</td>\n<td>8 (44.4%)</td>\n<td>2 (28.6%)</td>\n<td>6 (54.5%)</td>\n<td></td>\n</tr>\n<tr>\n<td>CD86 expression</td>\n<td></td>\n<td></td>\n<td></td>\n<td>0.066</td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Positive</td>\n<td>10 (55.6%)</td>\n<td>6 (85.7%)</td>\n<td>4 (36.4%)</td>\n<td></td>\n</tr>\n<tr>\n<td style=\"padding-left:2em;\">Negative</td>\n<td>8 (44.4%)</td>\n<td>1 (14.3%)</td>\n<td>7 (63.6%)</td>\n<td></td>\n</tr>\n</tbody>\n</table>\n</div>\n<div>\n<ul>\n<li> Abbreviations: CR, complete remission; Distal<sup>#</sup>, antrum, angle, or lower body; GCB, germinal center B-cell; <i>N</i>, number; Proximal<sup>&</sup>, middle body, upper body, fundus, or cardia; Tumor invasiveness*, gastric wall involvement was evaluated by endoscopic ultrasonography or computed tomography in 16 patients. </li>\n</ul>\n</div>\n<div></div>\n</div>\n<p>To our knowledge, this is the first prospective study to demonstrate that if HP can be successfully eradicated, a proportion of patients with early-stage (IE/IIE1) gastric “pure” DLBCLs can be cured by first-line HPE (antibiotics treatment). Although the current study included only 18 patients, it demonstrated that approximately 40%–50% of patients with early-stage gastric “pure” DLBCLs were cured by first-line HPE. Importantly, these patients remained lymphoma-free for a median duration of 69.2 months. These findings are important because, in our study, most patients diagnosed with gastric “pure” DLBCLs were older, had some age-related comorbidities, and were intolerant to conventional chemotherapy (CHOP)-associated adverse effects [<span>9</span>]. In addition, the current results indicated that waiting for 6 weeks to witness the tumor responses to HPE after initiating antibiotics did not influence the subsequent therapeutic efficacy of immunochemotherapy, such as R-CHOP. However, physicians should closely monitor the clinical symptoms and signs of patients, and immediately arrange for endoscopic examinations and abdominal CT scans if patients present with aggravated gastrointestinal symptoms within 6 weeks of starting initial antibiotics and during follow-up period for those who achieve PR after the first endoscopic examination.</p>\n<p>The results of a durable long-term remission of gastric “pure” DLBCLs after successful HPE in the current study were consistent with the results from our previous exploratory study and two other studies from Japan and Italy [<span>1-3</span>]. Cumulatively, these studies show that certain patients with early-stage gastric “pure” DLBCLs remain HP-dependent, and they can be cured by first-line antibiotics, thus eradicating HP. A retrospective study by Torisu et al. assessed the response of first-line HPE in 11 patients with gastric DLBCLs and reported that four of six (66.7%) patients with “pure” DLBCLs and three of five (60%) patients with gastric DLBCL(MALT)s achieved CR after HPE [<span>10</span>]. Additionally, Torisu et al. showed that the median time to CR in patients with CR was 16 weeks [<span>10</span>].</p>\n<p>The current study showed that the depth of invasion or perigastric lymph node involvement did not always lead to a loss of HP dependence. In our study, two patients with tumors invading the muscularis propria or serosa and two with perigastric lymph node involvement were cured by first-line HPE. Furthermore, CD86, a co-stimulatory marker [<span>6, 11</span>], was expressed in lymphoma cells of pre-HPE biopsy in patients with tumors involving the perigastric lymph node. Additionally, a correlation was observed between CD86 expression and CR status in these patients (CD86 expression; CR vs. non-CR: 85.7% [6/7] vs. 36.4% [4/11]; <i>p</i> = 0.066 [Table 1]; CR/PR vs. SD/PD: 80.0% [8/10] vs. 25.0% [2/8]; <i>p</i> = 0.054 [Table S4]; Figure S3). Although the mechanisms underlying the regression of “pure” DLBCLs with perigastric lymph nodes involvement are unclear, we hypothesized that the eradication of HP might possibly inhibit HP-specific tumor infiltrative T-cells and their interaction with co-stimulatory molecules, CD86, cytokines, or chemokines [<span>12</span>]. This, in turn, could inhibit the T-cell homing mechanisms and immune-related signaling from the stomach to the perigastric lymph nodes [<span>12-14</span>].</p>\n<p>Torisu et al. compared the gene expression profiles (on the basis of the PanCancer Immune Profiling Panel analyses) between patients with CR tumors and those with non-CR tumors among 11 patients with gastric DLBCLs who were administered first-line HPE [<span>10</span>]. The study showed that B-cell receptor- and NF-κB-related signaling genes were significantly upregulated in non-CR tumors [<span>10</span>]. Kiesewetter et al. showed that in HP-negative MALT lymphomas (most antibiotic-unresponsive tumors), the most common genetic mutations were present in NF-κB signaling-related molecules [<span>15</span>]. Importantly, our findings demonstrated that tumors expressing nuclear BCL10 or NF-κB (p65) were significantly associated with antibiotic unresponsiveness in patients who were administered first-line HPE. These findings suggest that a combination of both nuclear expression of BCL10 and NF-κB (p65) might predict non-CR status and allow physicians to administer immunochemotherapy at an early stage in these patients.</p>\n<p>In summary, the current prospective phase II study demonstrated that a proportion of patients with early-stage HP-positive gastric “pure” DLBCLs are HP-dependent and sufficiently responsive to first-line HPE, including patients with tumors invading the muscularis propria, serosa, or perigastric lymphatic areas. Furthermore, patients with gastric “pure” DLBCLs without CR were successfully treated with immunochemotherapy. Our findings suggest that a concise trial of HPE (to avoid potential adverse effects of immunochemotherapy) before immunochemotherapy is justified for patients whose stage IE1/IIE1 HP-positive gastric “pure” DLBCLs tumors do not express nuclear BCL10 or NF-κB (p65) because this patient subgroup is generally older than 70 years and can have comorbidities.</p>","PeriodicalId":7724,"journal":{"name":"American Journal of Hematology","volume":"42 1","pages":""},"PeriodicalIF":10.1000,"publicationDate":"2025-02-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Hematology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/ajh.27624","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Our exploratory study evaluated the efficacy of first-line Helicobacter pylori eradication (HPE) therapy on early-stage (stage IE/IIE1) Helicobacter pylori (HP)-positive gastric diffuse large B-cell lymphomas (DLBCLs) without histological evidence of mucosa-associated lymphoid tissue (MALT) (“pure” DLBCLs). The study showed that 11 of 16 (68.8%) patients achieved complete remission (CR) after successful HPE and remained lymphoma-free after a median follow-up of 7.7 years [1]. Another study by Tari et al. demonstrated that 4 of 15 (26.7%) patients with gastric “pure” DLBCLs who received first-line antibiotic treatment achieved CR and remained lymphoma-free after a median follow-up of 7–100 months [2]. Additionally, Ferrieri et al. studied 16 patients with gastric DLBCLs, of whom, 11 had “pure” DLBCLs and five had DLBCLs with histological evidence of MALT (DLBCL[MALT]), who were administered HPE (including clarithromycin, tinidazole or metronidazole, and omeprazole) [3]. Of these, eight patients achieved CR and three achieved partial remission (PR), with an overall response rate (ORR) of 68.8% after HPE [3]. Cumulatively, these findings indicate that certain patients with gastric “pure” DLBCLs are responsive to first-line antibiotic therapy and might have a better quality of life because they are not exposed to the conventional immunochemotherapy-related adverse effects. However, prospective studies evaluating patients whose tumors are not limited to the stomach but extend to the perigastric lymph node area are warranted.
Considering that “pure” DLBCLs of the stomach grow rapidly when the tumors do not respond to first-line HPE, identifying molecular markers that can predict HP independence (the lack of CR of tumors after completing HPE) is necessary. Our previous study showed that in in vitro DLBCL cell lines, B cell activating factor (BAFF) triggered the activation of NF-κB. Furthermore, it caused nuclear translocation of BCL10 by inducing AKT phosphorylation and disrupting the interaction of BCL10 with MALT1 and subsequent complex formation of BCL10 and BCL3 (nuclei translation-related genes) [4]. Furthermore, in tumor samples from patients with gastric DLBCL(MALT)s who received first-line HPE, BAFF overexpression was significantly associated with the nuclear translocation of BCL10 or NF-κB (p65), and the aforementioned molecules (including BAFF, nuclear BCL10, and nuclear NF-κB (p65)) were significantly correlated with HP independence of the tumor [4]. In contrast to HP-independent biomarkers, we detected HP-encoded protein cytotoxin-associated gene A (CagA) in tumor samples of patients with gastric MALT lymphomas and DLBCL(MALT)s [5, 6]. The expression of CagA was more frequent in HP-dependent tumors than in HP-independent tumors of gastric lymphomas [5, 6].
In March 2015, the National Taiwan University and the National Health Research Institutes of Taiwan initiated a prospective phase II, multicenter trial named the Taiwan Cooperative Oncology Group (TCOG) 2214 trial, registered at ClinicalTrials.gov (NCT02388581). This trial assessed the treatment efficacy of first-line HPE treatment and the predictivity of the HP-dependent marker—CagA and of HP-independent markers—BAFF and nuclear expression of BCL10 or NF-κB (p65)—in early-stage (stages IE and IIE1) HP-positive gastric “pure” DLBCLs. Patients who had histologically confirmed stage IE and IIE1 primary gastric “pure” DLBCLs and had no prior chemotherapy or radiotherapy for his/her gastric “pure” DLBCLs were enrolled. Detailed information on histological diagnosis and criteria of “pure” DLBCL, staging work-up, diagnosis of HP infection, HPE regimen, clinical follow-up, and the histological scoring system of the Groupe d'Etude des Lymphomes de l'Adult (GELA) [7] for assessing lymphoma responses toward HPE are provided in Supplementary Methods. The experimental methods for immunohistochemical detection of CagA, BCL10, NF-κB (p65), BAFF, CD10, BCL6, and MUM-1, interphase fluorescence in situ hybridization for assessing t(11;18)(q21;q21), primary endpoints, secondary endpoints, and statistical analyses are provided in the Supplementary Methods [6, 8]. All patients provided written informed consent for follow-ups and agreed to provide pathological samples for translational studies. All experimental protocols were approved by the Institutional Review Board (IRB) of the Research Ethical Committee of the National Taiwan University Hospital (NTUH) (NTUH IRB numbers: 201411005MINA).
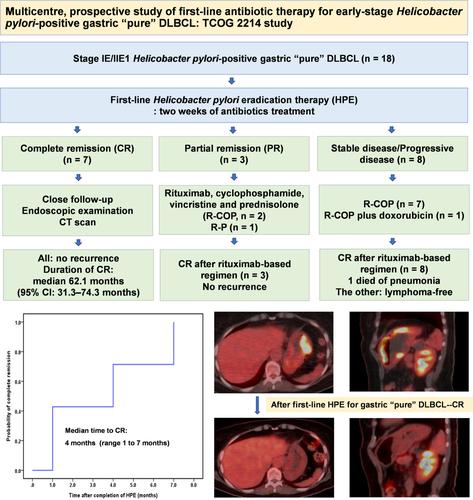
Between March 2015 and September 2020, a total of 18 patients with stage IE/IIE1 HP-positive gastric “pure” DLBCLs who met the eligibility criteria were recruited. The cohort comprised eight men and 10 women (median age, 66 years; range, 23–89 years). Among them, 15 patients were diagnosed with HP infection based on a positive histological examination or rapid urease test, and three had a positive 13C urea breath test. The most common symptom was epigastric discomfort. Before participating in the clinical trial, two patients had undergone 1 week of HPE regimen for treating ulcers and gastric discomforts. These two patients were diagnosed with HP infection (one based on histology examination and the other based on 13C urea breath test) before starting our HPE regimen protocol. The clinicopathological features of the enrolled 18 patients are outlined in Table S1. Initially, HP infection was successfully eradicated in two of five (40%) patients after they underwent first-line sequential HPE regimen (Figure S1). After shifting to quadruple antibiotic therapy (Figure 1A), 12 of 13 (92.3%), patients achieved successful HPE. Four patients with “pure” DLBCLs exhibited persistent HP infection after the first-line antibiotic therapy and were subsequently, immediately treated with systemic immunochemotherapy for avoiding progressive disease (PD) (Figure 1A). Grade 1 adverse effects such as nausea, diarrhea, and constipation were reported in patients administered with HPE regimens. No adverse effects of grades 2, 3, or 4 were reported.
FIGURE 1
Open in figure viewerPowerPoint
The schema, clinical courses, and clinical outcomes of first-line Helicobacter pylori eradication therapy (HPE) for stage IE/IIE1 gastric “pure” DLBCL. (A) The schema for bismuth quadruple HPE regimen, biological markers, follow-up, and salvage treatment if no response to HPE. (B) Time to CR in seven patients with gastric “pure” DLBCLs, as calculated from the completion of antibiotic treatment to the first evidence of CR through Kaplan–Meier analysis. (C) Duration of CR, time to chemotherapy for patients without CR, relapse status, survival, and ongoing status of all patients. *: The presence of HP infection is defined as a positive result, based on biopsy, histology, rapid urease test, 13C urea breath test, serology, or culture. **: The presence of t(11;18)(q21;q21) was assessed by the interphase fluorescence in situ hybridization (FISH) method using a commercially available probe (BIRC3/MALT1 dual-color, dual-fusion translocation probe; Vysis LSI/Abbott). The expressions of BCL10, NF-κB (p65), BAFF, and CagA were assessed by immunohistochemistry (IHC). Abbreviation: CR, complete remission; PR, partial remission; SD, stable disease; PD, progressive disease.
Of the 18 patients administered with first-line HPE, seven (38.9%) achieved CR and three (16.7%) achieved PR, with an ORR of 55.6% (95% confidence interval [CI], 30.1%–80.9%) determined based on the criteria of the GELA scoring system. Figure 2 illustrates alterations in the endoscopic findings and histological characteristics in a representative case of CR. In the 14 patients who achieved successful HP eradication, first-line HPE resulted in an ORR of 71.4% (CR = 7 [50.0%], PR = 3 [21.4%]; 95% CI, 44.3%–98.5%). The median time to CR after completion of HPE for all patients (n = 7) who achieved CR was 4.00 months (95% CI, 0.49–7.51 months; range 1–7 months) (Figure 1B). All seven patients who achieved CR after HPE were alive and DLBCL-free, and the median CR duration was 69.2 months (95% CI, 34.8–103.6 months; range, 38.4–81.4 months) (Figure 1C). Figure 3A–E present alterations in endoscopic examination findings and 18F-FDG PET/CT image findings for representative patients with CR, with long-term CR after completion of HPE.
FIGURE 2
Open in figure viewerPowerPoint
Endoscopic and histopathological manifestations in a patient with gastric “pure” DLBCLs who completely responded to first-line Helicobacter pylori eradication therapy (HPE). (A) Before HPE, multiple larger ulcerative lesions with elevated and swelling borders up to 4 cm in diameter are found at the antrum, angle, and lower body of the stomach (Endoscopic ultrasonography [EUS] showing tumor with involvement of muscularis propria layers [maximum thickness: 14.1 mm], left bottom inset). One month after completing HPE, three protruding ulcerative tumors are found at the antrum and lower body of stomach, and partial remission (PR) is achieved (EUS, maximum thickness: 12.6 mm, left bottom inset). Four months after completing HPE, two protruding tumors with improved ulceration and continued PR are found at the antrum of stomach (EUS, maximum thickness: 8.5 mm, right upper inset). Seven months after completing HPE, complete remission (CR) of ulcerative mass with hyperemic patches is observed at the antrum of the stomach (EUS, right upper inset). (B) A CT scan performed before HPE shows gastric wall thickness at the antrum and lower body of the stomach (axial and coronal view, white arrow). Four months after completing HPE, PR of gastric wall thickness is observed (coronal view, white arrow), and CR is observed at 7 months after completion of HPE (coronal view, white arrow). (C) Before HPE, hematoxylin and eosin stain (H&E) staining (upper panel 100×; lower panel 400×): Biopsy of ulcerative mass of antrum shows diffuse large lymphoid cells (enlarged nuclei and vesicular chromatin pattern) infiltrating the lamina propria (right upper inset, large cells are positive for CD20). Four months after completing HPE, H&E staining (upper panel 100×; lower panel 400×) shows immunoblast-like large lymphoid cells infiltrating the lamina propria. Seven months after completing HPE, H&E staining (upper panel 100×; lower panel 400×) shows chronic gastritis with lymphoplasma cells infiltration in the mucosal glands and lamina propria.
FIGURE 3
Open in figure viewerPowerPoint
Endoscopic examination and 18F-FDG PET/CT examination of a patient with long-term CR after first-line HPE, and survival curve of all patients with gastric “pure” DLBCLs who received first-line HPE. (A) Endoscopy shows enlarged gastric folds with multiple nodularity and ulceration (the largest one was found 2 cm in size in the middle body) at the greater curvature of gastric lower body, extending to the greater curvature of the gastric upper body in an 73-year-old woman before HPE (histopathology revealed “pure” DLBCL without histological evidence of mucosa-associated lymphoid tissue). (B) A PET/CT reveals intense hot areas (white arrow) along the greater curvature of the gastric wall (standard uptake value max = 34.19) (axial, coronal, and sagittal views). (C) The patient achieved CR 7 months after completing HPE, as documented by endoscopic examination and histologic manifestations. (D) At 17 months after completion of HPE, endoscopy shows CR with gastritis and scattered scars in the middle body of the stomach in the same case presented in (A). (E) At 24 months after completing HPE, PET/CT reveals still CR with completely resolved prior gastric lymphoma in the same case presented in (A) (Deauville score = 2). (F) The event-free survival curve and the overall survival for all cases. Abbreviations: PET, positron emission tomography; CT, computed tomography; CR, complete remission; HPE, Helicobacter pylori eradication therapy; EFS, event-free survival; OS, overall survival.
In the current study, among patients without CR (n = 11), most were older (age range 58–89 years, except for one patient who was 23 years old) and had age-related comorbidities. Considering their elderly status and comorbidities and that these patients may be intolerant to conventional chemotherapy (CHOP, cyclophosphamide, doxorubicin, vincristine, and prednisolone)-associated adverse effects, patients without CR were treated with a rituximab (R)-based regimen (most R-COP [cyclophosphamide, vincristine, and prednisolone], except for one patient who was 89 years old and was treated with rituximab plus prednisolone [RP], and one patient [23 years] received R-CHOP). The information on age and age-related comorbidities of patients with gastric “pure” DLBCL who received a rituximab (R)-based regimen after failing to completely respond to frontline HPE regimens is listed in Table S2. Three patients achieved PR at the first follow-up conducted 1 month after completing HPE and were administered subsequent immunochemotherapy consisting of R-COP (n = 2) or RP (n = 1) at 7, 9, and 10 months for the first, second, and third patient, respectively, because of progressive symptoms and disease during follow-up of endoscopic or abdominal CT scan examinations (Figure 1A,C). Notably, these three patients achieved CR after being administered immunochemotherapy. Of the eight patients who did not respond to HPE (stable disease [SD], n = 5; PD, n = 3), seven were treated with R-COP and one with R-CHOP; all of them subsequently achieved CR (Figure 1A,C). After a median follow-up of 61.1 months (95% CI; 46.3–75.9 months; range 7.0–103.1 months), only one patient died from pneumonia unrelated to lymphoma. Another patient who exhibited initial PD after HPE and achieved CR after being administered R-COP, developed local relapse of gastric DLBCL after 2 years and again achieved CR after being administered R-CHOP (Figure 1C). The 5-year event-free survival rate for all patients was 88.9% (95% CI, 74.4%–100%), and the 5-year overall survival rate for all patients was 94.4% (95% CI, 83.8%–100%) (Figure 3F).
The main clinicopathological features of the seven patients who achieved CR and the 11 who did not, and their responses to HPE are summarized in Table 1. No statistically significant differences were observed for age, sex, endoscopic appearance, stage, or tumor location between patients with CR and non-CR tumors. Tumor size < 5 cm (endoscopic extended maximal size) (p = 0.05) and tumor invasion less than the muscularis propria (p = 0.063) were associated with CR status (Table 1). Nuclear BCL10 expression (p = 0.004), nuclear NF-κB (p65) expression (p = 0.004), and BAFF expression (p = 0.0498) were significantly associated with non-CR status, whereas GCB subtype was not associated with CR status (according to the Hans algorithm) (Table 1, Figures S2 and S3A,B). However, we found no significant differences of CagA expression, nuclear BCL10 expression, nuclear NF-κB (p65) expression, and BAFF expression in tumor cells between patients with CR and those with PR (Table S3). When we classified our patients as those with responsive tumors (CR and PR, n = 10) and those with non-responsive tumors (SD and PD, n = 8), we found that sex (p = 0.025), tumor size < 5 cm (p = 0.015), presence of CagA expression (p = 0.023), absence of nuclear expression of BCL10 (p = 0.003) and NF-κB (p65) (p = 0.003), and BAFF expression (p = 0.015) were significantly associated with the tumor response to HPE (Table S4).
TABLE 1. Differential clinicopathologic features and molecular markers between patients with CR and those without CR tumors.
Characteristics
Total (N = 18)
CR-tumors (N = 7)
Non-CR tumors (N = 11)
p
Age
0.447
Median (range)
66.5 (23–89)
67.0 (36–73)
66.0 (23–89)
Sex
0.145
Women
10 (55.6%)
2 (28.6%)
8 (72.7%)
Men
8 (44.4%)
5 (71.4%)
3 (27.3%)
Endoscopic appearance
0.605
Ulcerative lesion
14 (77.8%)
5 (71.4%)
9 (81.8%)
Non-ulcerative lesion
4 (22.2%)
2 (28.1%)
2 (18.2%)
Location
0.620
Proximal&
6 (33.7%)
1 (14.3%)
5 (45.5%)
Distal#
12 (67.3%)
6 (85.7%)
6 (54.5%)
Tumor size
0.050
≥ 5 cm
9 (50.0%)
1 (14.3%)
8 (72.7%)
< 5 cm
9 (50.0%)
6 (85.7%)
3 (27.3%)
Stage
0.605
IE1
14 (77.8%)
5 (71.4%)
9 (81.8%)
IIE1
4 (22.2%)
2 (28.6%)
2 (18.2%)
Tumor invasiveness*
0.063
Mucosa/submucosa
3 (18.8%)
3 (42.9%)
0 (0.0%)
Muscularis/serosa/IIE1
13 (81.2%)
4 (57.1%)
9 (100%)
CagA expression
0.119
Positive
14 (77.8%)
7 (100%)
7 (63.6%)
Negative
4 (22.2%)
0 (0.0%)
4 (36.4%)
Nuclear BCL10 expression
0.004
Positive
8 (44.4%)
0 (0.0%)
8 (72.7%)
Negative
10 (55.6%)
7 (100%)
3 (27.3%)
Nuclear NF-κB (p65) expression
0.004
Positive
8 (44.4%)
0 (0.0%)
8 (72.7%)
Negative
10 (55.6%)
7 (100%)
3 (27.3%)
BAFF overexpression
0.0498
Positive
9 (50%)
1 (14.3%)
8 (72.7%)
Negative
9 (50%)
6 (85.7%)
3 (27.3%)
GCB/non-GCB
0.367
GCB
10 (55.6%)
5 (71.4%)
5 (45.5%)
Non-GCB
8 (44.4%)
2 (28.6%)
6 (54.5%)
CD86 expression
0.066
Positive
10 (55.6%)
6 (85.7%)
4 (36.4%)
Negative
8 (44.4%)
1 (14.3%)
7 (63.6%)
Abbreviations: CR, complete remission; Distal#, antrum, angle, or lower body; GCB, germinal center B-cell; N, number; Proximal&, middle body, upper body, fundus, or cardia; Tumor invasiveness*, gastric wall involvement was evaluated by endoscopic ultrasonography or computed tomography in 16 patients.
To our knowledge, this is the first prospective study to demonstrate that if HP can be successfully eradicated, a proportion of patients with early-stage (IE/IIE1) gastric “pure” DLBCLs can be cured by first-line HPE (antibiotics treatment). Although the current study included only 18 patients, it demonstrated that approximately 40%–50% of patients with early-stage gastric “pure” DLBCLs were cured by first-line HPE. Importantly, these patients remained lymphoma-free for a median duration of 69.2 months. These findings are important because, in our study, most patients diagnosed with gastric “pure” DLBCLs were older, had some age-related comorbidities, and were intolerant to conventional chemotherapy (CHOP)-associated adverse effects [9]. In addition, the current results indicated that waiting for 6 weeks to witness the tumor responses to HPE after initiating antibiotics did not influence the subsequent therapeutic efficacy of immunochemotherapy, such as R-CHOP. However, physicians should closely monitor the clinical symptoms and signs of patients, and immediately arrange for endoscopic examinations and abdominal CT scans if patients present with aggravated gastrointestinal symptoms within 6 weeks of starting initial antibiotics and during follow-up period for those who achieve PR after the first endoscopic examination.
The results of a durable long-term remission of gastric “pure” DLBCLs after successful HPE in the current study were consistent with the results from our previous exploratory study and two other studies from Japan and Italy [1-3]. Cumulatively, these studies show that certain patients with early-stage gastric “pure” DLBCLs remain HP-dependent, and they can be cured by first-line antibiotics, thus eradicating HP. A retrospective study by Torisu et al. assessed the response of first-line HPE in 11 patients with gastric DLBCLs and reported that four of six (66.7%) patients with “pure” DLBCLs and three of five (60%) patients with gastric DLBCL(MALT)s achieved CR after HPE [10]. Additionally, Torisu et al. showed that the median time to CR in patients with CR was 16 weeks [10].
The current study showed that the depth of invasion or perigastric lymph node involvement did not always lead to a loss of HP dependence. In our study, two patients with tumors invading the muscularis propria or serosa and two with perigastric lymph node involvement were cured by first-line HPE. Furthermore, CD86, a co-stimulatory marker [6, 11], was expressed in lymphoma cells of pre-HPE biopsy in patients with tumors involving the perigastric lymph node. Additionally, a correlation was observed between CD86 expression and CR status in these patients (CD86 expression; CR vs. non-CR: 85.7% [6/7] vs. 36.4% [4/11]; p = 0.066 [Table 1]; CR/PR vs. SD/PD: 80.0% [8/10] vs. 25.0% [2/8]; p = 0.054 [Table S4]; Figure S3). Although the mechanisms underlying the regression of “pure” DLBCLs with perigastric lymph nodes involvement are unclear, we hypothesized that the eradication of HP might possibly inhibit HP-specific tumor infiltrative T-cells and their interaction with co-stimulatory molecules, CD86, cytokines, or chemokines [12]. This, in turn, could inhibit the T-cell homing mechanisms and immune-related signaling from the stomach to the perigastric lymph nodes [12-14].
Torisu et al. compared the gene expression profiles (on the basis of the PanCancer Immune Profiling Panel analyses) between patients with CR tumors and those with non-CR tumors among 11 patients with gastric DLBCLs who were administered first-line HPE [10]. The study showed that B-cell receptor- and NF-κB-related signaling genes were significantly upregulated in non-CR tumors [10]. Kiesewetter et al. showed that in HP-negative MALT lymphomas (most antibiotic-unresponsive tumors), the most common genetic mutations were present in NF-κB signaling-related molecules [15]. Importantly, our findings demonstrated that tumors expressing nuclear BCL10 or NF-κB (p65) were significantly associated with antibiotic unresponsiveness in patients who were administered first-line HPE. These findings suggest that a combination of both nuclear expression of BCL10 and NF-κB (p65) might predict non-CR status and allow physicians to administer immunochemotherapy at an early stage in these patients.
In summary, the current prospective phase II study demonstrated that a proportion of patients with early-stage HP-positive gastric “pure” DLBCLs are HP-dependent and sufficiently responsive to first-line HPE, including patients with tumors invading the muscularis propria, serosa, or perigastric lymphatic areas. Furthermore, patients with gastric “pure” DLBCLs without CR were successfully treated with immunochemotherapy. Our findings suggest that a concise trial of HPE (to avoid potential adverse effects of immunochemotherapy) before immunochemotherapy is justified for patients whose stage IE1/IIE1 HP-positive gastric “pure” DLBCLs tumors do not express nuclear BCL10 or NF-κB (p65) because this patient subgroup is generally older than 70 years and can have comorbidities.
期刊介绍:
The American Journal of Hematology offers extensive coverage of experimental and clinical aspects of blood diseases in humans and animal models. The journal publishes original contributions in both non-malignant and malignant hematological diseases, encompassing clinical and basic studies in areas such as hemostasis, thrombosis, immunology, blood banking, and stem cell biology. Clinical translational reports highlighting innovative therapeutic approaches for the diagnosis and treatment of hematological diseases are actively encouraged.The American Journal of Hematology features regular original laboratory and clinical research articles, brief research reports, critical reviews, images in hematology, as well as letters and correspondence.




 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


