{"title":"Muscular Injury Is a Risk Factor for Post-Entire Circumferential Esophageal Endoscopic Submucosal Dissection Stricture.","authors":"Daisuke Azuma, Kingo Hirasawa, Reo Atsusaka, Yuichiro Ozeki, Atsushi Sawada, Masafumi Nishio, Ryosuke Kobayashi, Chiko Sato, Shin Maeda","doi":"10.1159/000543846","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Endoscopic submucosal dissection (ESD) has become a widely adopted treatment for early esophageal cancer. However, extensive mucosal defects resulting from ESD pose a significant risk of post-procedural strictures. Despite efforts to prevent strictures through various means, including steroid administration, they remain a challenge, significantly impacting patients' quality of life and healthcare costs. Thus, identifying risk factors for refractory strictures following entire circumferential esophageal ESD (EC-E-ESD) is imperative.</p><p><strong>Methods: </strong>Between July 2013 and September 2023, 49 patients who underwent EC-E-ESD were retrospectively analyzed. Patients were classified based on the presence of refractory or non-refractory strictures. A refractory stricture was defined as requiring six or more endoscopic balloon dilation procedures before stricture improvement. Clinicopathological features and outcomes were examined using multivariate logistic regression analysis.</p><p><strong>Results: </strong>Refractory strictures were observed in 51% of patients. A comparison showed that the refractory group had a significantly higher percentage of muscular injury (52% vs. 8%, p = 0.002) and mucosal defect length ≥50 mm (68% vs. 37%, p = 0.047) than the non-refractory group. Multivariate analysis showed that muscular injury (odds ratio 16.2; 95% confidence interval: 2.04-129.1) was an independent risk factor for refractory strictures after EC-E-ESD.</p><p><strong>Conclusions: </strong>Muscular injury during EC-E-ESD is a risk factor for refractory strictures. Strategies to prevent injury, such as meticulous dissection techniques and effective steroid administration, may mitigate this risk. However, current prophylactic measures are inadequate, highlighting the need for further research into preventive strategies.</p><p><strong>Introduction: </strong>Endoscopic submucosal dissection (ESD) has become a widely adopted treatment for early esophageal cancer. However, extensive mucosal defects resulting from ESD pose a significant risk of post-procedural strictures. Despite efforts to prevent strictures through various means, including steroid administration, they remain a challenge, significantly impacting patients' quality of life and healthcare costs. Thus, identifying risk factors for refractory strictures following entire circumferential esophageal ESD (EC-E-ESD) is imperative.</p><p><strong>Methods: </strong>Between July 2013 and September 2023, 49 patients who underwent EC-E-ESD were retrospectively analyzed. Patients were classified based on the presence of refractory or non-refractory strictures. A refractory stricture was defined as requiring six or more endoscopic balloon dilation procedures before stricture improvement. Clinicopathological features and outcomes were examined using multivariate logistic regression analysis.</p><p><strong>Results: </strong>Refractory strictures were observed in 51% of patients. A comparison showed that the refractory group had a significantly higher percentage of muscular injury (52% vs. 8%, p = 0.002) and mucosal defect length ≥50 mm (68% vs. 37%, p = 0.047) than the non-refractory group. Multivariate analysis showed that muscular injury (odds ratio 16.2; 95% confidence interval: 2.04-129.1) was an independent risk factor for refractory strictures after EC-E-ESD.</p><p><strong>Conclusions: </strong>Muscular injury during EC-E-ESD is a risk factor for refractory strictures. Strategies to prevent injury, such as meticulous dissection techniques and effective steroid administration, may mitigate this risk. However, current prophylactic measures are inadequate, highlighting the need for further research into preventive strategies.</p>","PeriodicalId":11294,"journal":{"name":"Digestive Diseases","volume":" ","pages":"125-134"},"PeriodicalIF":2.1000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11965824/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000543846","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/3 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Endoscopic submucosal dissection (ESD) has become a widely adopted treatment for early esophageal cancer. However, extensive mucosal defects resulting from ESD pose a significant risk of post-procedural strictures. Despite efforts to prevent strictures through various means, including steroid administration, they remain a challenge, significantly impacting patients' quality of life and healthcare costs. Thus, identifying risk factors for refractory strictures following entire circumferential esophageal ESD (EC-E-ESD) is imperative.
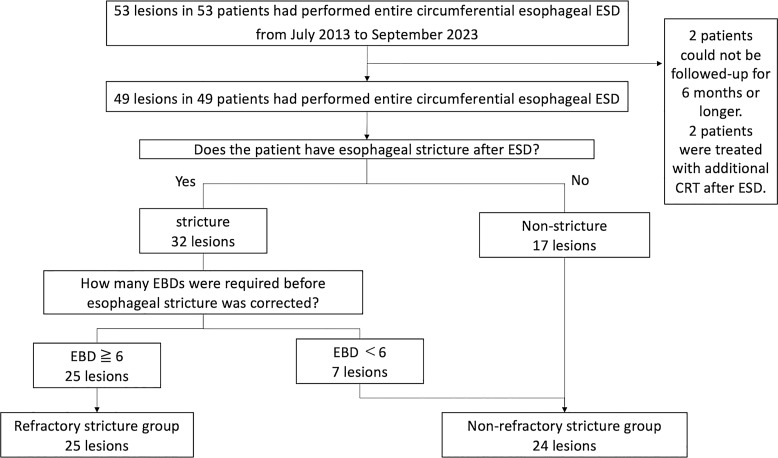
Methods: Between July 2013 and September 2023, 49 patients who underwent EC-E-ESD were retrospectively analyzed. Patients were classified based on the presence of refractory or non-refractory strictures. A refractory stricture was defined as requiring six or more endoscopic balloon dilation procedures before stricture improvement. Clinicopathological features and outcomes were examined using multivariate logistic regression analysis.
Results: Refractory strictures were observed in 51% of patients. A comparison showed that the refractory group had a significantly higher percentage of muscular injury (52% vs. 8%, p = 0.002) and mucosal defect length ≥50 mm (68% vs. 37%, p = 0.047) than the non-refractory group. Multivariate analysis showed that muscular injury (odds ratio 16.2; 95% confidence interval: 2.04-129.1) was an independent risk factor for refractory strictures after EC-E-ESD.
Conclusions: Muscular injury during EC-E-ESD is a risk factor for refractory strictures. Strategies to prevent injury, such as meticulous dissection techniques and effective steroid administration, may mitigate this risk. However, current prophylactic measures are inadequate, highlighting the need for further research into preventive strategies.
Introduction: Endoscopic submucosal dissection (ESD) has become a widely adopted treatment for early esophageal cancer. However, extensive mucosal defects resulting from ESD pose a significant risk of post-procedural strictures. Despite efforts to prevent strictures through various means, including steroid administration, they remain a challenge, significantly impacting patients' quality of life and healthcare costs. Thus, identifying risk factors for refractory strictures following entire circumferential esophageal ESD (EC-E-ESD) is imperative.
Methods: Between July 2013 and September 2023, 49 patients who underwent EC-E-ESD were retrospectively analyzed. Patients were classified based on the presence of refractory or non-refractory strictures. A refractory stricture was defined as requiring six or more endoscopic balloon dilation procedures before stricture improvement. Clinicopathological features and outcomes were examined using multivariate logistic regression analysis.
Results: Refractory strictures were observed in 51% of patients. A comparison showed that the refractory group had a significantly higher percentage of muscular injury (52% vs. 8%, p = 0.002) and mucosal defect length ≥50 mm (68% vs. 37%, p = 0.047) than the non-refractory group. Multivariate analysis showed that muscular injury (odds ratio 16.2; 95% confidence interval: 2.04-129.1) was an independent risk factor for refractory strictures after EC-E-ESD.
Conclusions: Muscular injury during EC-E-ESD is a risk factor for refractory strictures. Strategies to prevent injury, such as meticulous dissection techniques and effective steroid administration, may mitigate this risk. However, current prophylactic measures are inadequate, highlighting the need for further research into preventive strategies.
内镜下粘膜剥离术(ESD)已成为早期食管癌广泛采用的治疗方法。然而,由ESD引起的广泛粘膜缺损会造成术后狭窄的重大风险。尽管通过各种手段(包括类固醇管理)努力预防狭窄,但它们仍然是一个挑战,严重影响患者的生活质量和医疗保健费用。因此,确定全周食管ESD (EC-E-ESD)后难治性狭窄的危险因素是必要的。方法:回顾性分析2013年7月至2023年9月49例接受EC-E-ESD手术的患者。根据是否存在难治性或非难治性狭窄对患者进行分类。难治性狭窄定义为在狭窄改善前需要6次或以上的内镜球囊扩张(EBD)手术。采用多变量logistic回归分析检查临床病理特征和结果。结果:顽固性狭窄占51%。比较发现,难治组肌肉损伤比例(52% vs. 8%, p=0.002)和粘膜缺损长度≥50 mm (68% vs. 37%, p=0.047)明显高于非难治组。多因素分析显示肌肉损伤(优势比16.2;95%可信区间:2.04-129.1)是EC-E-ESD术后难治性狭窄的独立危险因素。结论:EC-E-ESD术中肌肉损伤是难治性狭窄的危险因素。预防损伤的策略,如细致的解剖技术和有效的类固醇给药,可以减轻这种风险。然而,目前的预防措施是不够的,这突出表明需要进一步研究预防战略。
期刊介绍:
Each issue of this journal is dedicated to a special topic of current interest, covering both clinical and basic science topics in gastrointestinal function and disorders. The contents of each issue are comprehensive and reflect the state of the art, featuring editorials, reviews, mini reviews and original papers. These individual contributions encompass a variety of disciplines including all fields of gastroenterology. ''Digestive Diseases'' bridges the communication gap between advances made in the academic setting and their application in patient care. The journal is a valuable service for clinicians, specialists and physicians-in-training.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


