Surgical Outcomes Stratified by Type of Transportation and Presence of Coronary Reperfusion in Patients with Coronary Malperfusion Caused by Type A Aortic Dissection.
{"title":"Surgical Outcomes Stratified by Type of Transportation and Presence of Coronary Reperfusion in Patients with Coronary Malperfusion Caused by Type A Aortic Dissection.","authors":"Kazuki Noda, Yosuke Inoue, Yoshimasa Seike, Hitoshi Matsuda","doi":"10.5761/atcs.oa.24-00182","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Owing to the time-sensitive nature of myocardial ischemia, challenging clinical scenarios should be considered in patients with type A acute aortic dissection (AAAD) complicated by coronary malperfusion. In clinical settings, the diagnosis and reperfusion strategies for coronary malperfusion often depend on institutional resources. This study evaluated early surgical outcomes in such patients, focusing on transportation type and clinical management.</p><p><strong>Methods: </strong>We retrospectively reviewed 70 patients who underwent emergency surgery for AAAD with coronary malperfusion, excluding those with cardiac tamponade on arrival, between 1997 and February 2024. Patients were divided into 2 groups based on transportation: direct transfer and referral.</p><p><strong>Results: </strong>Overall, in-hospital mortality was 27%, with only 1 of 9 patients surviving with preoperative peripheral extracorporeal membrane oxygenation (ECMO). Mortality and morbidity did not significantly differ between groups. Univariate analysis identified left coronary artery involvement and preoperative hemodynamic instability as significant risk factors. Additionally, preoperative diagnostic-only coronary angiography (CAG) with unsuccessful reperfusion was a potential risk factor (P = 0.06).</p><p><strong>Conclusions: </strong>Regardless of transportation type, preoperative peripheral ECMO itself could not be a definitive solution in AAAD patients with coronary malperfusion. Also, patients who underwent preoperative CAG with unsuccessful reperfusion might be fatal, especially with suspected left coronary artery involvement.</p>","PeriodicalId":93877,"journal":{"name":"Annals of thoracic and cardiovascular surgery : official journal of the Association of Thoracic and Cardiovascular Surgeons of Asia","volume":"31 1","pages":""},"PeriodicalIF":1.3000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11873597/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of thoracic and cardiovascular surgery : official journal of the Association of Thoracic and Cardiovascular Surgeons of Asia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5761/atcs.oa.24-00182","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Owing to the time-sensitive nature of myocardial ischemia, challenging clinical scenarios should be considered in patients with type A acute aortic dissection (AAAD) complicated by coronary malperfusion. In clinical settings, the diagnosis and reperfusion strategies for coronary malperfusion often depend on institutional resources. This study evaluated early surgical outcomes in such patients, focusing on transportation type and clinical management.
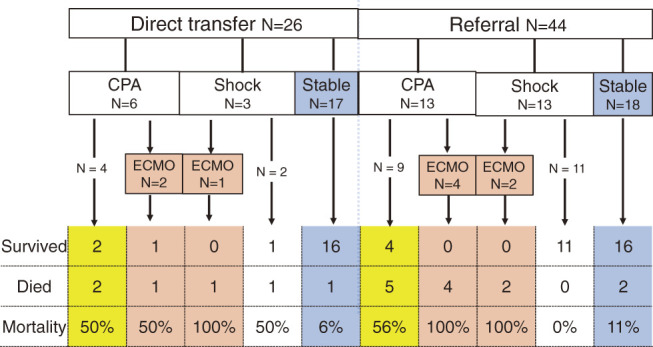
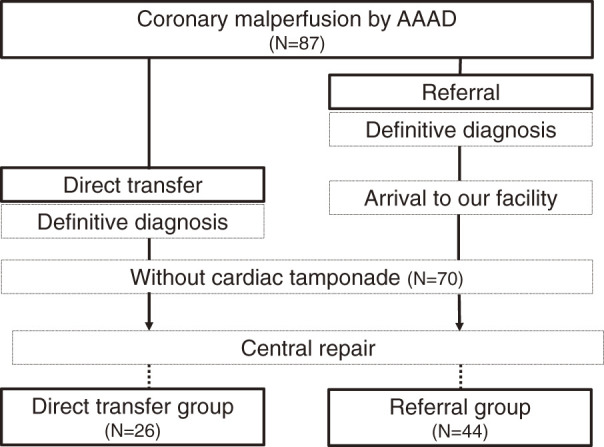
Methods: We retrospectively reviewed 70 patients who underwent emergency surgery for AAAD with coronary malperfusion, excluding those with cardiac tamponade on arrival, between 1997 and February 2024. Patients were divided into 2 groups based on transportation: direct transfer and referral.
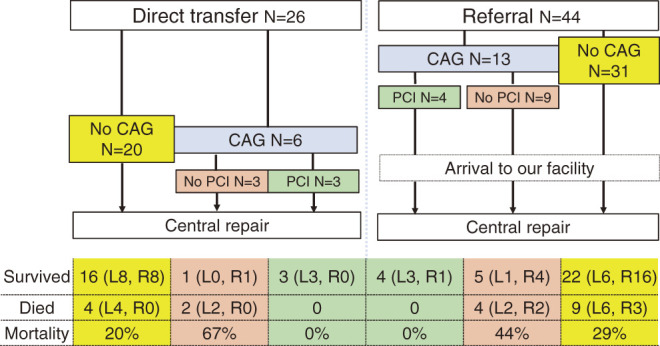
Results: Overall, in-hospital mortality was 27%, with only 1 of 9 patients surviving with preoperative peripheral extracorporeal membrane oxygenation (ECMO). Mortality and morbidity did not significantly differ between groups. Univariate analysis identified left coronary artery involvement and preoperative hemodynamic instability as significant risk factors. Additionally, preoperative diagnostic-only coronary angiography (CAG) with unsuccessful reperfusion was a potential risk factor (P = 0.06).
Conclusions: Regardless of transportation type, preoperative peripheral ECMO itself could not be a definitive solution in AAAD patients with coronary malperfusion. Also, patients who underwent preoperative CAG with unsuccessful reperfusion might be fatal, especially with suspected left coronary artery involvement.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


