{"title":"Mortality and factors associated with acute exacerbation after non-cardiac surgery in patients with interstitial pneumonia: a retrospective study.","authors":"Kaoru Umehara, Kazuhiro Shirozu, Taichi Ando, Kentaro Tokuda, Kei Makishima, Kazuya Imura, Shota Tsumura, Shinnosuke Takamori, Ken Yamaura","doi":"10.4097/kja.24656","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute exacerbation of interstitial pneumonia (AE-IP) is associated with high mortality rates. Although the risk factors for AE-IP have been extensively studied, given the small sample sizes, only a few risk factors have been established. This study aimed to investigate the postoperative mortality and factors associated with AE-IP.</p><p><strong>Methods: </strong>This retrospective study included 482 patients with a preoperative diagnosis of IP who underwent noncardiac surgery between December 2012 and April 2020. AE-IP was diagnosed by a radiologist using computed tomography when worsening respiratory symptoms were observed within 1 month postoperatively. The Cox proportional hazards model was used to compare mortality rates. Candidate factors associated with AE-IP were identified through logistic regression analysis using the variable selection method, followed by case-control analysis using propensity score matching to determine possible factors associated with AE-IP.</p><p><strong>Results: </strong>The multivariable-adjusted hazard ratios for all-cause and IP-related deaths were significantly higher in patients with AE-IP than in those without AE-IP. Multivariable analysis with variable selection suggested that male sex, higher C-reactive protein (CRP) levels, fraction of inspired oxygen (FiO2) ≥ 60%, and non-lung surgery were candidate factors associated with AE-IP. Case-control analysis using propensity score matching demonstrated that patients with AE-IP had higher CRP levels (P = 0.044) and frequency of FiO2 ≥ 60% (P = 0.035) than those without AE-IP. Furthermore, a positive, nearly linear relationship was observed between FiO2 ≥ 60% duration and AE-IP incidence.</p><p><strong>Conclusions: </strong>Intraoperative management with FiO2 ≥ 60% and high preoperative CRP levels were significantly associated with postoperative AE-IP.</p>","PeriodicalId":17855,"journal":{"name":"Korean Journal of Anesthesiology","volume":" ","pages":"453-461"},"PeriodicalIF":6.3000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12489585/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Anesthesiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4097/kja.24656","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/3 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Acute exacerbation of interstitial pneumonia (AE-IP) is associated with high mortality rates. Although the risk factors for AE-IP have been extensively studied, given the small sample sizes, only a few risk factors have been established. This study aimed to investigate the postoperative mortality and factors associated with AE-IP.
Methods: This retrospective study included 482 patients with a preoperative diagnosis of IP who underwent noncardiac surgery between December 2012 and April 2020. AE-IP was diagnosed by a radiologist using computed tomography when worsening respiratory symptoms were observed within 1 month postoperatively. The Cox proportional hazards model was used to compare mortality rates. Candidate factors associated with AE-IP were identified through logistic regression analysis using the variable selection method, followed by case-control analysis using propensity score matching to determine possible factors associated with AE-IP.
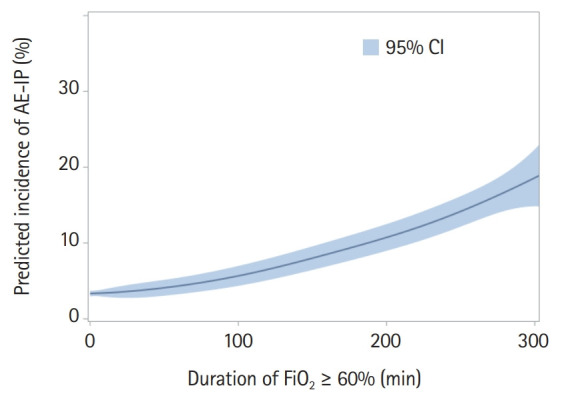
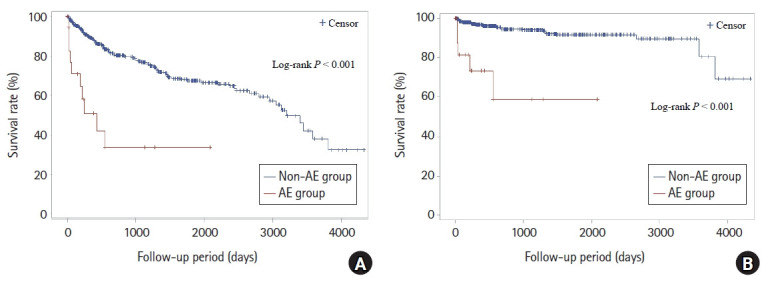
Results: The multivariable-adjusted hazard ratios for all-cause and IP-related deaths were significantly higher in patients with AE-IP than in those without AE-IP. Multivariable analysis with variable selection suggested that male sex, higher C-reactive protein (CRP) levels, fraction of inspired oxygen (FiO2) ≥ 60%, and non-lung surgery were candidate factors associated with AE-IP. Case-control analysis using propensity score matching demonstrated that patients with AE-IP had higher CRP levels (P = 0.044) and frequency of FiO2 ≥ 60% (P = 0.035) than those without AE-IP. Furthermore, a positive, nearly linear relationship was observed between FiO2 ≥ 60% duration and AE-IP incidence.
Conclusions: Intraoperative management with FiO2 ≥ 60% and high preoperative CRP levels were significantly associated with postoperative AE-IP.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


