Regional cerebral oxygen saturation during initial mobilization of critically ill patients is associated with clinical outcomes: a prospective observational study.
{"title":"Regional cerebral oxygen saturation during initial mobilization of critically ill patients is associated with clinical outcomes: a prospective observational study.","authors":"Ryota Imai, Takafumi Abe, Kentaro Iwata, Seigo Yamaguchi, Takeshi Kitai, Atsuhiro Tsubaki","doi":"10.1186/s40635-025-00722-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Vital signs help determine the safety of early mobilization in critically ill patients in intensive care units. However, none of these variables directly assess cerebral circulation. Therefore, we aimed to investigate the relationship of regional cerebral oxygen saturation (rSO<sub>2</sub>) and vital signs with in-hospital death in critically ill patients.</p><p><strong>Methods: </strong>This prospective study included critically ill patients admitted to the Uonuma Kikan Hospital Emergency Center who received physical therapy between June 2020 and December 2022. We continuously measured rSO<sub>2</sub> during the initial mobilization using a wearable brain near-infrared spectroscopy device. With in-hospital death as the primary endpoint, the association between rSO<sub>2</sub> and in-hospital death was assessed in Analysis 1 to determine the rSO<sub>2</sub> cut-off value that predicts in-hospital death. In Analysis 2, patients were categorised into survival and non-survival groups to examine the temporal changes in vital signs and rSO<sub>2</sub> associated with postural changes during mobilization.</p><p><strong>Results: </strong>Of the 132 eligible patients, 98 were included in Analysis 1, and 70 were included in Analysis 2. Analysis 1 demonstrated that lower premobilization rSO<sub>2</sub> was independently associated with in-hospital death (odds ratio 0.835, 95% confidence interval 0.724-0.961, p = 0.012). Receiver operating characteristic curve analysis identified an optimal rSO<sub>2</sub> cut-off value of 57% for predicting in-hospital death (area under the curve 0.818, sensitivity 73%, specificity 83%). Analysis 2 showed that rSO<sub>2</sub> changes during mobilization were unrelated to changes in vital signs, suggesting rSO<sub>2</sub> as an independent prognostic marker.</p><p><strong>Conclusions: </strong>The results suggest that rSO<sub>2</sub> measured during initial mobilization is associated with in-hospital death in critically ill patients.</p>","PeriodicalId":13750,"journal":{"name":"Intensive Care Medicine Experimental","volume":"13 1","pages":"13"},"PeriodicalIF":2.8000,"publicationDate":"2025-02-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11790542/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intensive Care Medicine Experimental","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40635-025-00722-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Vital signs help determine the safety of early mobilization in critically ill patients in intensive care units. However, none of these variables directly assess cerebral circulation. Therefore, we aimed to investigate the relationship of regional cerebral oxygen saturation (rSO2) and vital signs with in-hospital death in critically ill patients.
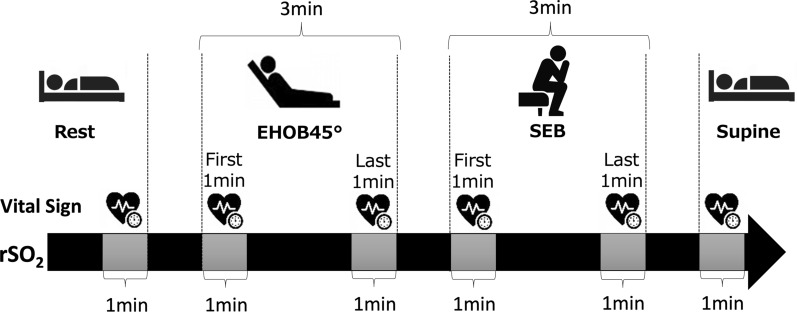
Methods: This prospective study included critically ill patients admitted to the Uonuma Kikan Hospital Emergency Center who received physical therapy between June 2020 and December 2022. We continuously measured rSO2 during the initial mobilization using a wearable brain near-infrared spectroscopy device. With in-hospital death as the primary endpoint, the association between rSO2 and in-hospital death was assessed in Analysis 1 to determine the rSO2 cut-off value that predicts in-hospital death. In Analysis 2, patients were categorised into survival and non-survival groups to examine the temporal changes in vital signs and rSO2 associated with postural changes during mobilization.
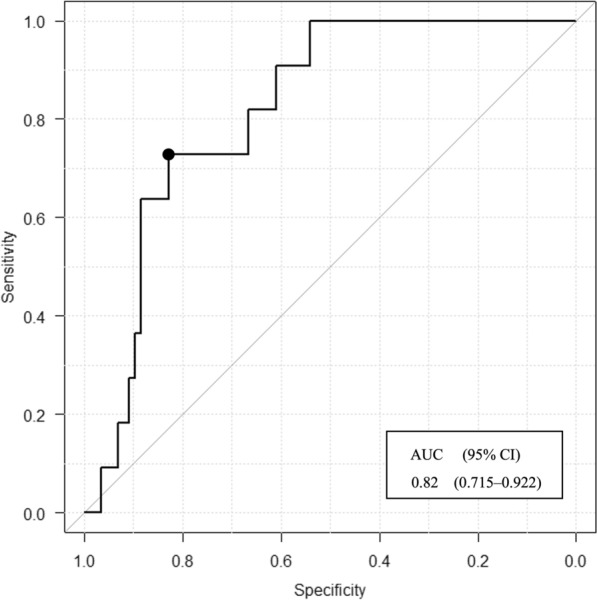
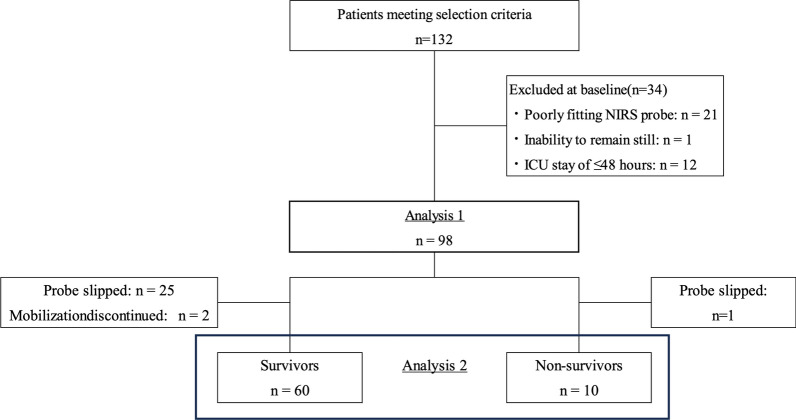
Results: Of the 132 eligible patients, 98 were included in Analysis 1, and 70 were included in Analysis 2. Analysis 1 demonstrated that lower premobilization rSO2 was independently associated with in-hospital death (odds ratio 0.835, 95% confidence interval 0.724-0.961, p = 0.012). Receiver operating characteristic curve analysis identified an optimal rSO2 cut-off value of 57% for predicting in-hospital death (area under the curve 0.818, sensitivity 73%, specificity 83%). Analysis 2 showed that rSO2 changes during mobilization were unrelated to changes in vital signs, suggesting rSO2 as an independent prognostic marker.
Conclusions: The results suggest that rSO2 measured during initial mobilization is associated with in-hospital death in critically ill patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


