Hypogonadism in a Man With Cystic Fibrosis and an Unusually Low Serum Testosterone: A Cautionary Tale
IF 1.2
Q3 Medicine
引用次数: 0
Abstract
Background/Objective
Men with cystic fibrosis (CF) have a high prevalence of low testosterone levels. A recent retrospective study demonstrated a quarter of a cohort of men with CF had serum testosterone levels below 300 ng/dL. The evaluation of hypogonadism is of increasing clinical importance in order to prevent unfavorable outcomes. Herein we present a 31-year-old man with CF and a relatively low serum testosterone value who was found to have an additional unsuspected cause of male hypogonadism.
Case Report
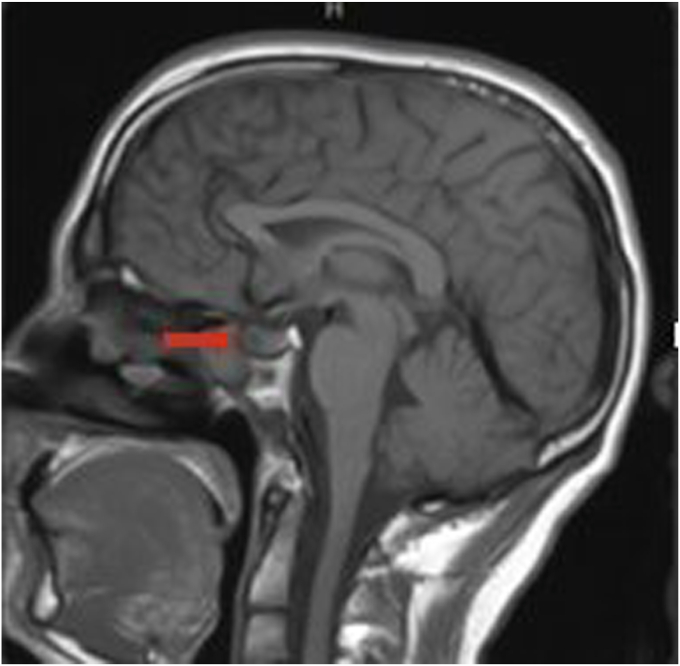
The patient was a 31-year-old man with history of CF who was referred to endocrinology clinic for the evaluation of hypogonadism. Serum testing revealed a total testosterone of 175 ng/mL (296-1377), luteinizing hormone 2.8 mIU/mL (1.2-8.6), and a prolactin of 341 ng/mL (3-13). A brain magnetic resonance imaging was obtained, which revealed a 1 cm hypoenhancing left sellar lesion. He was started on cabergoline. His testosterone increased to 707 ng/dL after a year on cabergoline treatment. His prolactin decreased to 12 ng/mL after a year of treatment. The pituitary adenoma decreased 50% in size 2 years after cabergoline was initiated.
Discussion
The most common etiologies of CF are recurrent infections, chronic inflammation, and glucocorticoid administration, which lead to both hypothalamic-pituitary dysregulation and primary hypogonadism. However, other less common causes of hypogonadism can also be found in CF.
Conclusion
We suggest that all men with cystic fibrosis found to have hypogonadism undergo additional evaluation for causes of hypogonadism prior to treatment with testosterone.

囊性纤维化和血清睾酮异常低的男性性腺功能减退:一个警世故事。
背景/目的:囊性纤维化(CF)患者睾酮水平低的患病率很高。最近的一项回顾性研究表明,四分之一的CF患者血清睾酮水平低于300 ng/dL。评估性腺功能减退症是越来越重要的临床,以防止不良后果。在这里,我们提出了一个31岁的男性CF和相对较低的血清睾酮值谁被发现有一个额外的男性性腺功能减退症的未知原因。病例报告:患者为31岁男性,既往有CF病史,因性腺功能减退被转介至内分泌科门诊。血清检测显示总睾酮175 ng/mL(296-1377),促黄体生成素2.8 mIU/mL(1.2-8.6),催乳素341 ng/mL(3-13)。脑磁共振成像显示左鞍区1厘米低增强病灶。他开始服用卡麦角林。卡麦角林治疗一年后,他的睾酮水平上升至707 ng/dL。治疗1年后催乳素降至12 ng/mL。卡麦角林治疗2年后垂体腺瘤体积减小50%。讨论:CF最常见的病因是反复感染、慢性炎症和糖皮质激素的使用,这导致下丘脑-垂体失调和原发性性腺功能减退。然而,其他不常见的性腺功能减退的原因也可以在cf中发现。结论:我们建议所有患有囊性纤维化的男性发现有性腺功能减退,在使用睾酮治疗之前,对性腺功能减退的原因进行额外的评估。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

AACE Clinical Case Reports
Medicine-Endocrinology, Diabetes and Metabolism
CiteScore
2.30
自引率
0.00%
发文量
61
审稿时长
55 days
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


