Finding the Culprit: Cushing Syndrome Secondary to Lung Carcinoid Tumor
IF 1.2
Q3 Medicine
引用次数: 0
Abstract
Background/Objective
Cushing syndrome resulting from ectopic adrenocorticotropic hormone (ACTH) secretion (EAS) is a rare condition, and its occurrence in adolescents is even more uncommon, representing <1% of cases. We describe a case of EAS from a lung carcinoid tumor leading to Cushing syndrome in a young woman, which was successfully treated with excision of the tumor.
Case Report
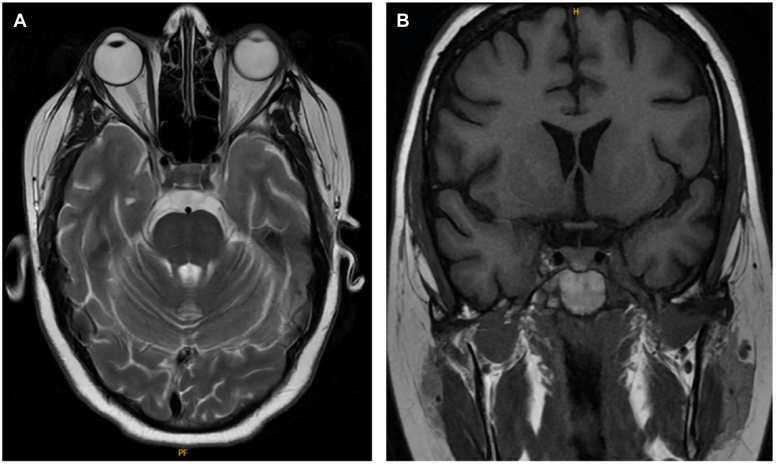
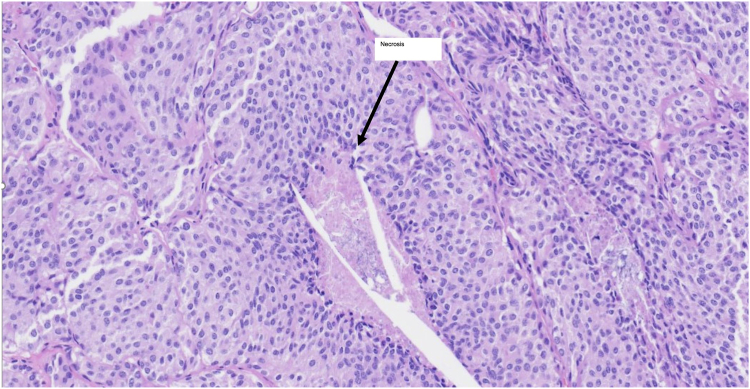
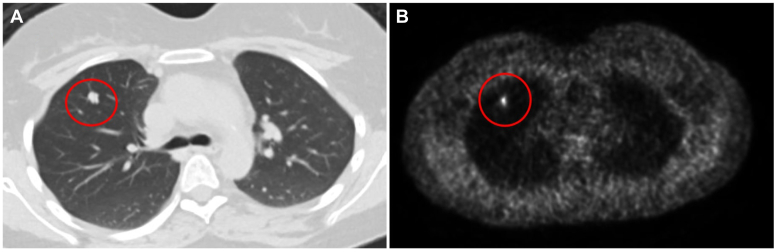
An 18-year-old woman presented with mood disturbances, weight gain, and fatigue for 6 months. Workup revealed high levels of urinary free cortisol (>900 μg/dL; normal range, <45 μg/dL) and midnight salivary cortisol (0.755 μg/dL; normal range, <0.09 μg/dL). The ACTH and cortisol levels remained elevated after a low-dose dexamethasone suppression test. Magnetic resonance imaging of the pituitary gland did not reveal any adenoma and inferior petrosal sinus sampling showed no central-to-peripheral gradient. A diagnosis of EAS was made. Subsequent body imaging noted a 1-cm lung nodule. Due to symptoms of severe hypercortisolism including hypokalemia and worsening mood changes, the patient was started on metyrapone as a bridge to surgery. A few weeks later, the patient underwent successful surgical resection, after which symptoms promptly resolved. Pathology report later confirmed an atypical lung carcinoid tumor. The patient remained in remission at 1-year follow-up.
Discussion
Medical therapy aids in managing severe hypercortisolism in ACTH-secreting tumors until definitive surgical treatment can be undertaken.
Conclusion
This case underscores the critical importance of promptly recognizing EAS and the resulting severe hypercortisolism symptoms because early surgical intervention can lead to a cure.
寻找罪魁祸首:继发于类肺癌的库欣综合征。
背景/目的:由促肾上腺皮质激素(ACTH)异位分泌(EAS)引起的库欣综合征是一种罕见的疾病,在青少年中发生更为罕见,代表病例报告:一名18岁女性,表现为情绪障碍,体重增加和疲劳6个月。检查显示尿中游离皮质醇水平高(约900 μg/dL;讨论:药物治疗有助于控制acth分泌肿瘤的严重高皮质醇症,直到可以进行明确的手术治疗。结论:本病例强调了及时识别EAS及其导致的严重高皮质醇血症症状的重要性,因为早期手术干预可以治愈。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

AACE Clinical Case Reports
Medicine-Endocrinology, Diabetes and Metabolism
CiteScore
2.30
自引率
0.00%
发文量
61
审稿时长
55 days
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


