{"title":"Colonic Dieulafoy Lesion as a Rare Cause of Lower Gastrointestinal Bleeding.","authors":"Mohamed Farag, Yordanka Diaz, Harish Patel","doi":"10.1159/000542790","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Dieulafoy lesion is one of the most under-recognized sources of gastrointestinal (GI) bleeding (GI), typically manifesting as acute upper gastrointestinal bleeding; endoscopy is usually the first diagnostic and therapeutic modality utilized to handle these lesions by employing a variety of procedures.</p><p><strong>Case report: </strong>This is a case of an 81-year-old female who was being assessed after experiencing repeated bouts of melena with hemoglobin drop. The patient had multiple comorbidities but no history of gastrointestinal bleeding. Esophagogastroduodenoscopy (EGD) revealed only Erythematous duodenopathy without active bleeding; the initial colonoscopy revealed a large amount of blood without identifying the source of bleeding; a second colonoscopy revealed classic Dieulafoy lesions in the splenic flexure, which were injected and clipped, and the bleeding ceased.</p><p><strong>Conclusion: </strong>Dieulafoy lesions are most frequently found in the stomach and gastroesophageal junction, but they have also been documented in other parts of the gastrointestinal tract. In this particular instance, the lesions were identified in the colon, which is an unusual location for them, and they were treated endoscopically by clipping and injecting. In conclusion, colonic Dieulafoy lesions, although rare, have the potential to cause life-threatening bleeding and should be included in the differential diagnosis of lower gastrointestinal bleeding.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"19 1","pages":"52-56"},"PeriodicalIF":0.6000,"publicationDate":"2025-01-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11785396/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000542790","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Dieulafoy lesion is one of the most under-recognized sources of gastrointestinal (GI) bleeding (GI), typically manifesting as acute upper gastrointestinal bleeding; endoscopy is usually the first diagnostic and therapeutic modality utilized to handle these lesions by employing a variety of procedures.
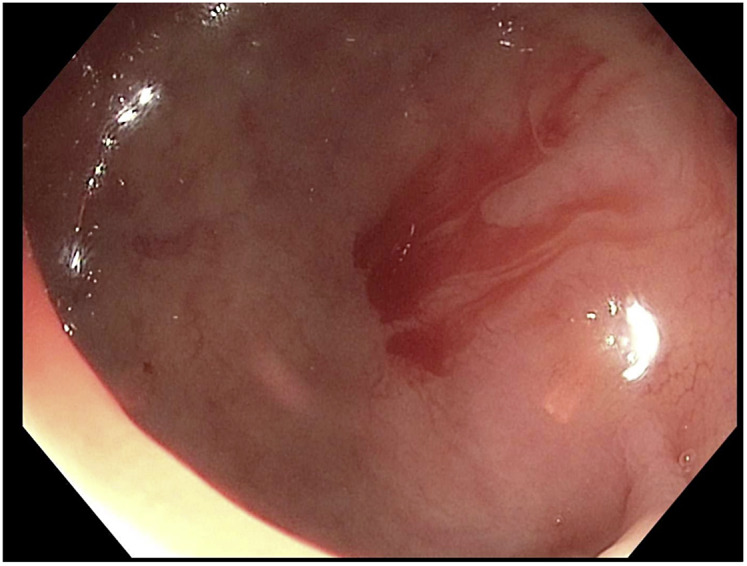
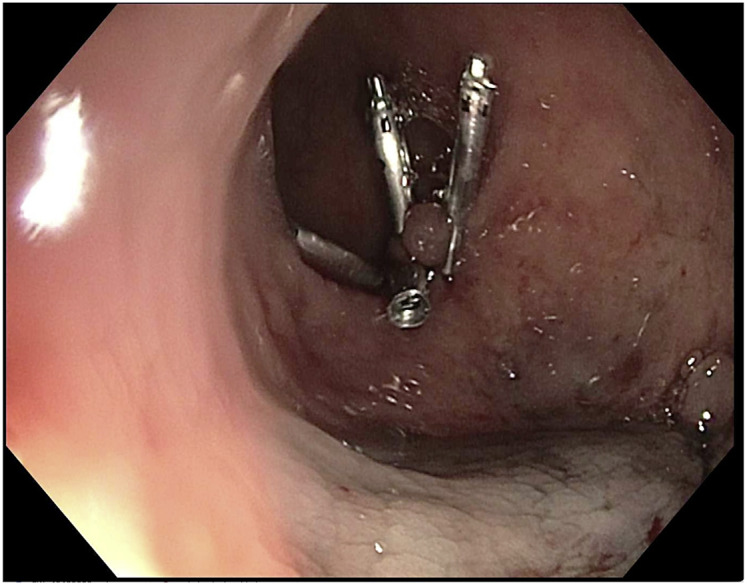
Case report: This is a case of an 81-year-old female who was being assessed after experiencing repeated bouts of melena with hemoglobin drop. The patient had multiple comorbidities but no history of gastrointestinal bleeding. Esophagogastroduodenoscopy (EGD) revealed only Erythematous duodenopathy without active bleeding; the initial colonoscopy revealed a large amount of blood without identifying the source of bleeding; a second colonoscopy revealed classic Dieulafoy lesions in the splenic flexure, which were injected and clipped, and the bleeding ceased.
Conclusion: Dieulafoy lesions are most frequently found in the stomach and gastroesophageal junction, but they have also been documented in other parts of the gastrointestinal tract. In this particular instance, the lesions were identified in the colon, which is an unusual location for them, and they were treated endoscopically by clipping and injecting. In conclusion, colonic Dieulafoy lesions, although rare, have the potential to cause life-threatening bleeding and should be included in the differential diagnosis of lower gastrointestinal bleeding.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


